Department of Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
J Gastric Cancer. 2011 Mar;11(1):31-7. doi: 10.5230/jgc.2011.11.1.31. Epub 2011 Mar 31.
We performed this study to evaluate the clinical presentation as well as the proper surgical intervention for ovarian metastasis from gastric cancers and these tumors were identified during postoperative follow-up. This will help establish the optimal strategy for improving the survival of patients with this entity.
22 patients (3.2%) with ovarian metastasis were noted when performing a retrospective chart review of (693) females patients who had undergone a resection for gastric cancer between 1981 and 2008. The covariates used for the survival analysis were the patient age at the time of ovarian relapse, the size of the tumor, the initial TNM stage of the gastric cancer, the interval to metastasis and the presence of gross residual disease after treatment for Krukenberg tumor. The cumulative survival curves for the patient groups were calculated with the Kaplan-Meier method and they were compared by means of the Log-Rank test.
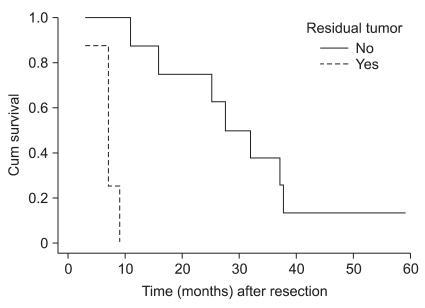
The average age of the patients was 48.6 years (range: 24 to 78 years) and the average survival time of the 22 patients was 18.8 months (the estimated 3-year survival rate was 15.8%) with a range of 2 to 59 months after the diagnosis of Krukenberg tumor. The survival rate for patients without gross residual disease was longer than that of the patients with gross residual disease (P=0.0003). In contrast, patient age, the size of ovarian tumor, the initial stage of gastric adenocarcinoma, the interval to metastasis and adjuvant chemotherapy were not prognostic indicators for survival after the development of ovarian metastasis.
Early diagnosis and complete resection are the only possible hope to improve survival. As the 3-year survival rate after resection of Krukenberg tumor is 15.8%, it seems worthwhile to consider performing tumorectomy as the second cytoreduction.
我们进行这项研究是为了评估胃癌术后随访中发现的卵巢转移的临床特征以及恰当的手术干预方法,以帮助制定改善此类患者生存的最佳策略。
回顾性分析 1981 年至 2008 年间 693 例行胃癌切除术的女性患者的病历,其中 22 例(3.2%)患者术后发生卵巢转移。生存分析的协变量包括卵巢复发时患者的年龄、肿瘤大小、胃癌的初始 TNM 分期、转移时间以及治疗克鲁肯伯格瘤后是否存在大体残留病灶。采用 Kaplan-Meier 法计算患者组的累积生存率,并采用 Log-Rank 检验进行比较。
患者的平均年龄为 48.6 岁(24 岁至 78 岁),22 例患者的平均生存时间为 18.8 个月(预计 3 年生存率为 15.8%),自诊断为克鲁肯伯格瘤后生存时间为 2 至 59 个月。无大体残留病灶患者的生存率长于有大体残留病灶患者(P=0.0003)。相比之下,患者年龄、卵巢肿瘤大小、胃癌的初始分期、转移时间和辅助化疗均不是发生卵巢转移后生存的预后指标。
早期诊断和完全切除是提高生存的唯一希望。由于克鲁肯伯格瘤切除后的 3 年生存率为 15.8%,因此考虑进行肿瘤切除术作为二线细胞减灭术似乎是值得的。