Rogers A D, Nel M, Eloff E P, Naidoo N G
Vascular Surgery Unit, Division of General Surgery, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa.
ISRN Surg. 2011;2011:819295. doi: 10.5402/2011/819295. Epub 2011 Apr 4.
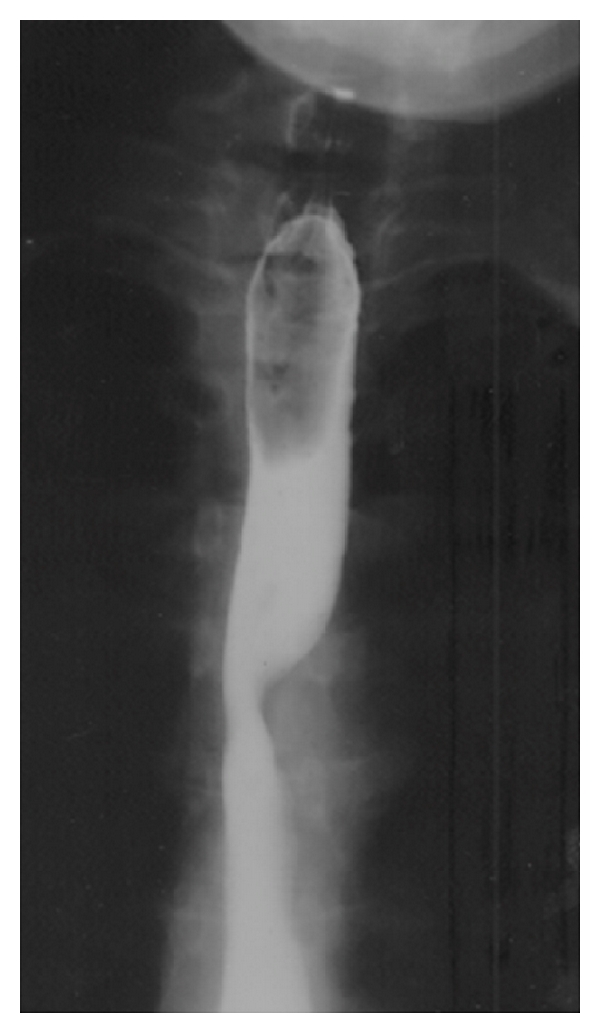
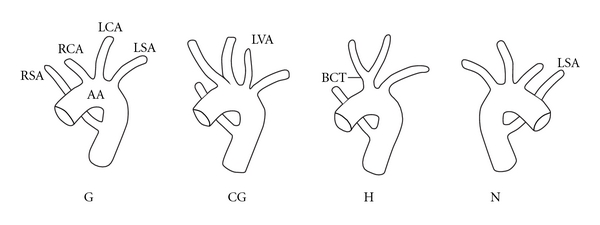
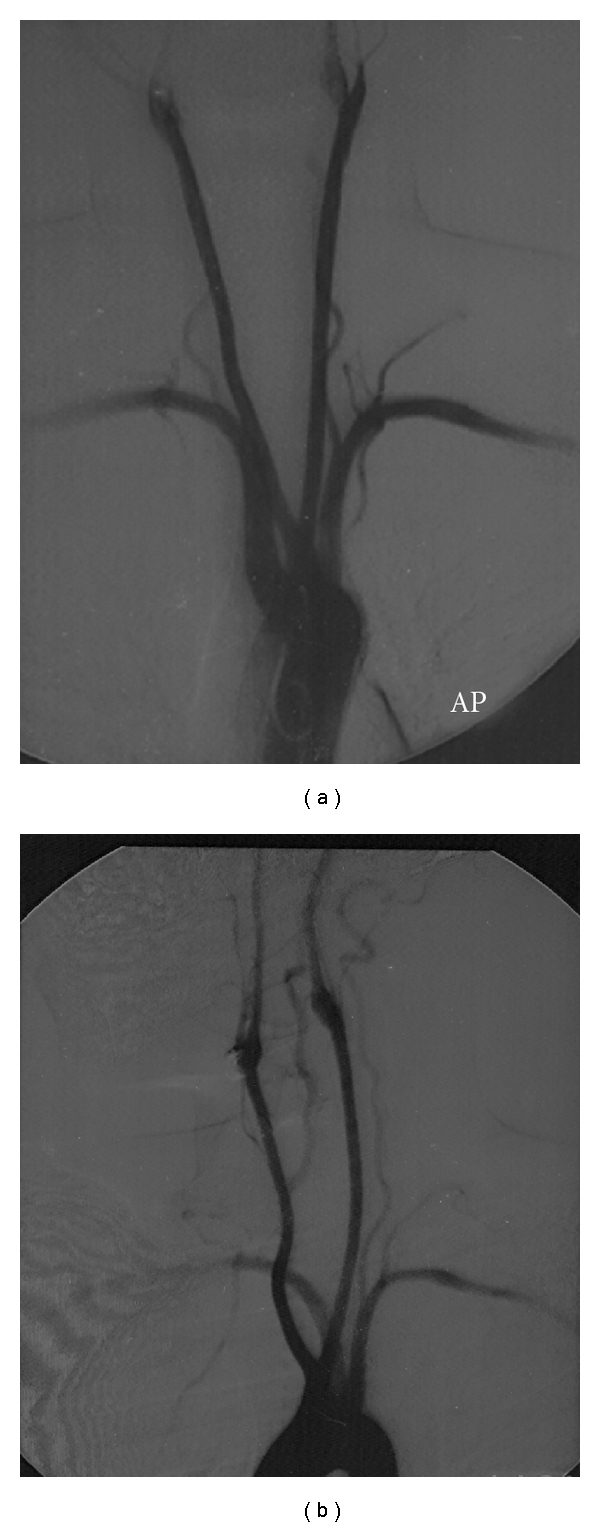
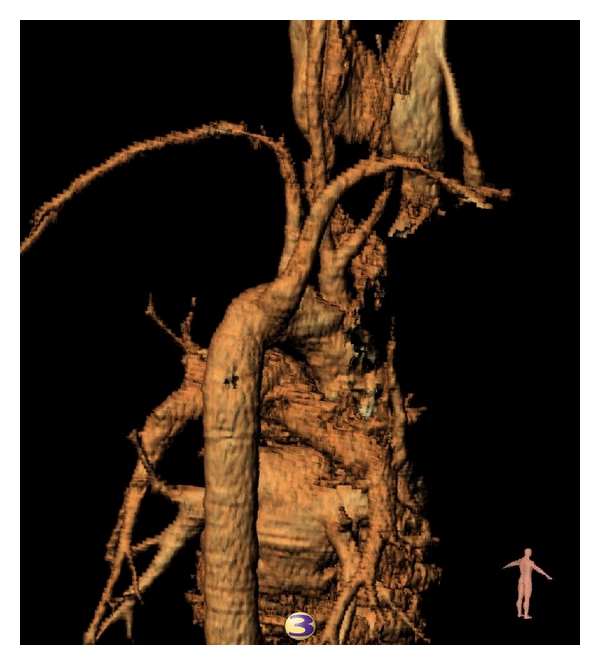
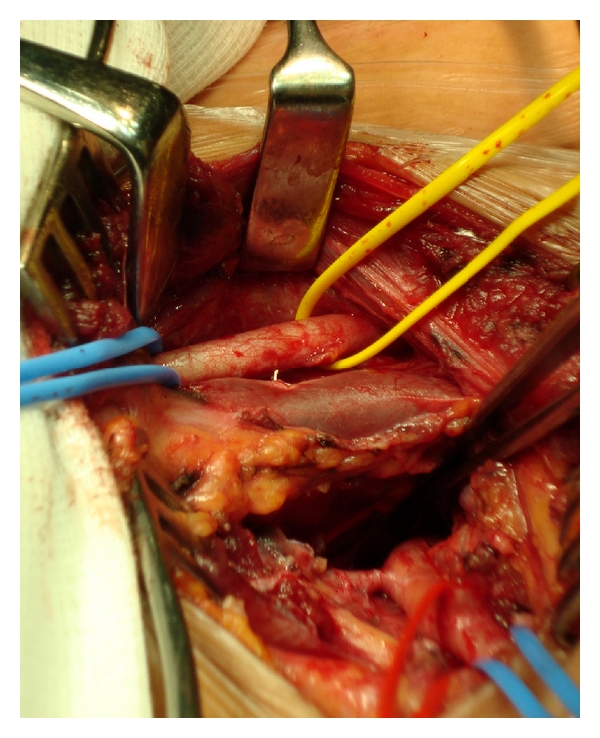
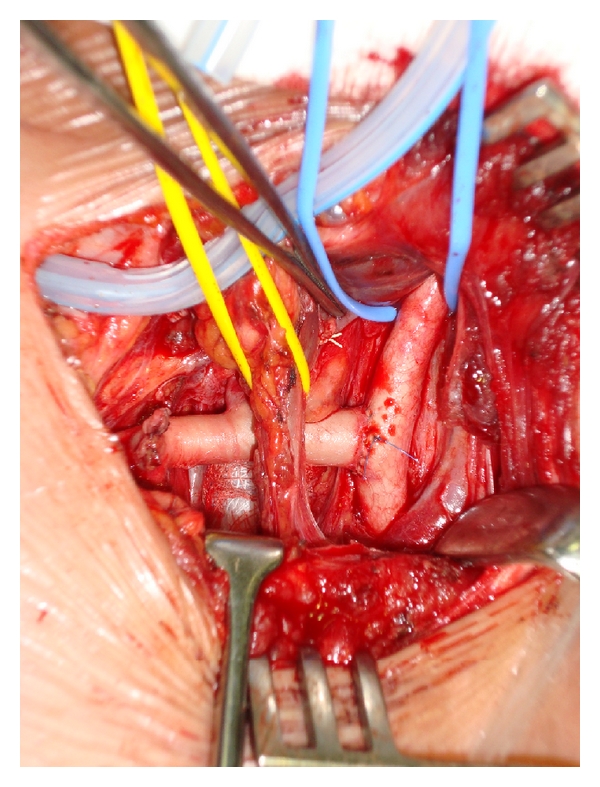
Dysphagia Lusoria is dysphagia secondary to an aberrant right subclavian artery that has a retroesophageal course. Adachi and Williams categorized aortic arch anomalies, showing that the right subclavian artery arising in this fashion (as the final branch of the descending aortic arch) is one of the more common. However, this very rarely coexists with a bicarotid trunk. We present such a case as it is manifested in a 36-year-old lady complaining of marked weight loss and dysphagia. The diagnosis remained elusive until a CT scan of the chest was performed; angiography further delineated the pathology. It is believed that the combination of the common carotid origins with the retroesophageal course of the aberrant vessel more frequently accounts for symptoms in the absence of an aneurysm of the origin of the aberrant vessel. Several techniques to manage the aberrant vessel have been described in the literature, but we favoured open ligation and transposition to the right carotid artery.
迷走右锁骨下动脉所致吞咽困难是指继发于走行于食管后方的迷走右锁骨下动脉的吞咽困难。安达奇和威廉姆斯对主动脉弓异常进行了分类,表明以这种方式起源的右锁骨下动脉(作为降主动脉弓的最后一个分支)是较为常见的情况之一。然而,这种情况很少与双颈动脉干并存。我们报告了这样一个病例,患者为一名36岁女性,主诉体重显著减轻和吞咽困难。在进行胸部CT扫描之前,诊断一直不明确;血管造影进一步明确了病变情况。据信,在异常血管起始处无动脉瘤的情况下,颈总动脉共同起源与异常血管走行于食管后方这一情况的组合更常导致症状出现。文献中描述了几种处理异常血管的技术,但我们倾向于采用开放结扎并将其转位至右颈动脉。