Child and Newborn Health Group, KEMRI-Wellcome Trust Research Programme, Nairobi, Kenya.
BMC Pediatr. 2011 Nov 25;11:109. doi: 10.1186/1471-2431-11-109.
There are few reports of interventions to reduce the common but irrational use of antibiotics for acute non-bloody diarrhoea amongst hospitalised children in low-income settings. We undertook a secondary analysis of data from an intervention comprising training of health workers, facilitation, supervision and face-to-face feedback, to assess whether it reduced inappropriate use of antibiotics in children with non-bloody diarrhoea and no co-morbidities requiring antibiotics, compared to a partial intervention comprising didactic training and written feedback only. This outcome was not a pre-specified end-point of the main trial.
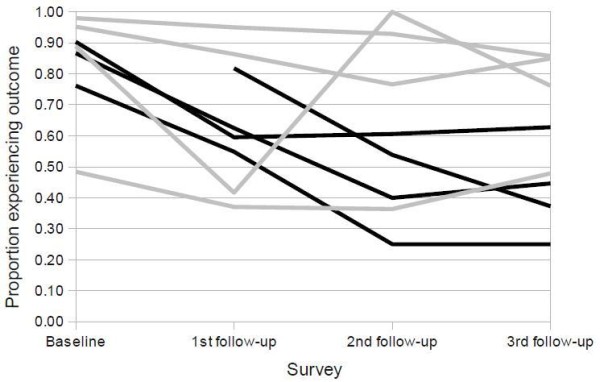
Repeated cross-sectional survey data from a cluster-randomised controlled trial of an intervention to improve management of common childhood illnesses in Kenya were used to describe the prevalence of inappropriate antibiotic use in a 7-day period in children aged 2-59 months with acute non-bloody diarrhoea. Logistic regression models with random effects for hospital were then used to identify patient and clinician level factors associated with inappropriate antibiotic use and to assess the effect of the intervention.
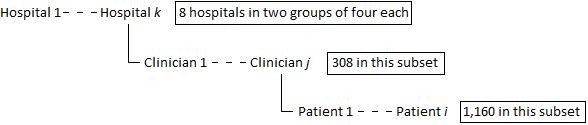
9, 459 admission records of children were reviewed for this outcome. Of these, 4, 232 (44.7%) were diagnosed with diarrhoea, with 130 of these being bloody (dysentery) therefore requiring antibiotics. 1, 160 children had non-bloody diarrhoea and no co-morbidities requiring antibiotics-these were the focus of the analysis. 750 (64.7%) of them received antibiotics inappropriately, 313 of these being in the intervention hospitals vs. 437 in the controls. The adjusted logistic regression model showed the baseline-adjusted odds of inappropriate antibiotic prescription to children admitted to the intervention hospitals was 0.30 times that in the control hospitals (95%CI 0.09-1.02).
We found some evidence that the multi-faceted, sustained intervention described in this paper led to a reduction in the inappropriate use of antibiotics in treating children with non-bloody diarrhoea.
International Standard Randomised Controlled Trial Number Register ISRCTN42996612.
在资源有限的环境中,针对住院儿童中常见但不合理使用抗生素治疗急性非血性腹泻的干预措施,相关报告较少。我们对一项包含卫生工作者培训、促进、监督和面对面反馈的干预措施的数据进行了二次分析,以评估与仅包含理论培训和书面反馈的部分干预措施相比,该干预措施是否可降低无合并症但需要抗生素治疗的非血性腹泻儿童中抗生素的不适当使用。这一结果并非主要试验的预先指定终点。
我们使用肯尼亚改善常见儿童疾病管理的一项干预措施的整群随机对照试验的重复横断面调查数据,描述了在 7 天内 2-59 月龄急性非血性腹泻儿童中抗生素使用不适当的发生率。然后,我们使用具有医院随机效应的逻辑回归模型,确定与抗生素使用不适当相关的患者和临床医生水平因素,并评估干预措施的效果。
共有 9459 份儿童住院记录用于评估该结果。其中,4232 例(44.7%)被诊断为腹泻,其中 130 例为血性(痢疾)腹泻,因此需要使用抗生素。160 例儿童患有非血性腹泻且无合并症需要使用抗生素,这是分析的重点。其中 750 例(64.7%)儿童不合理使用了抗生素,干预组 313 例,对照组 437 例。调整后的逻辑回归模型显示,与对照组相比,进入干预组的儿童不合理使用抗生素的可能性降低了 0.30 倍(95%CI 0.09-1.02)。
我们发现,与对照组相比,本文描述的多方面、持续的干预措施可能减少了非血性腹泻儿童抗生素的不适当使用。
国际标准随机对照试验注册处 ISRCTN42996612。