van Gils Paul F, Over Eelco A B, Hamberg-van Reenen Heleen H, de Wit G Ardine, van den Berg Matthijs, Schuit Albertine J, Engelfriet Peter M
National Institute for Public Health and the Environment, Centre for Prevention and Health Services Research, Bilthoven, the Netherlands.
BMJ Open. 2011 Dec 21;1(2):e000363. doi: 10.1136/bmjopen-2011-000363. Print 2011.
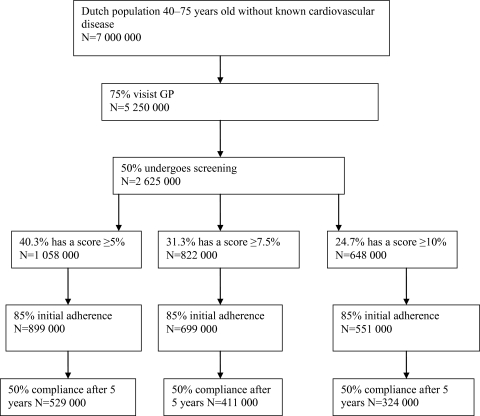
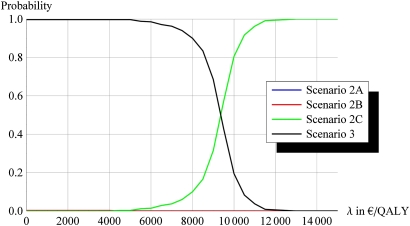
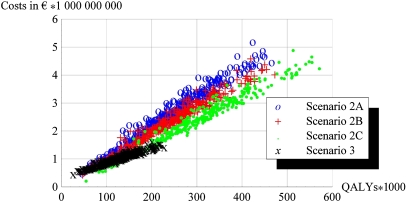
Objectives The aim of the present study was to estimate the cost-effectiveness of the polypill in the primary prevention of cardiovascular disease. Design A health economic modelling study. Setting Primary healthcare in the Netherlands. Participants Simulated individuals from the general Dutch population, aged 45-75 years. Interventions Opportunistic screening followed by prescription of the polypill to eligible individuals. Eligibility was defined as having a minimum 10-year risk of cardiovascular death as assessed with the Systematic Coronary Risk Evaluation function of alternatively 5%, 7.5% or 10%. Different versions of the polypill were considered, depending on composition: (1) the Indian polycap, with three different types of blood pressure-lowering drugs, a statin and aspirin; (2) as (1) but without aspirin and (3) as (2) but with a double statin dose. In addition, a scenario of (targeted) separate antihypertensive and/or statin medication was simulated. Primary outcome measures Cases of acute myocardial infarction or stroke prevented, quality-adjusted life years (QALYs) gained and the costs per QALY gained. All interventions were compared with usual care. Results All scenarios were cost-effective with an incremental cost-effectiveness ratio between €7900 and 12 300 per QALY compared with usual care. Most health gains were achieved with the polypill without aspirin and containing a double dose of statins. With a 10-year risk of 7.5% as the threshold, this pill would prevent approximately 3.5% of all cardiovascular events. Conclusions Opportunistic screening based on global cardiovascular risk assessment followed by polypill prescription to those with increased risk offers a cost-effective strategy. Most health gain is achieved by the polypill without aspirin and a double statin dose.
目的 本研究旨在评估复方制剂在心血管疾病一级预防中的成本效益。
设计 一项健康经济建模研究。
背景 荷兰的初级医疗保健。
参与者 模拟的45至75岁荷兰普通人群个体。
干预措施 机会性筛查,随后为符合条件的个体开具复方制剂。符合条件的定义为使用系统性冠状动脉风险评估功能评估的心血管死亡最低10年风险为5%、7.5%或10%。根据成分考虑了不同版本的复方制剂:(1)印度多效片,含有三种不同类型的降压药、一种他汀类药物和阿司匹林;(2)与(1)相同但不含阿司匹林;(3)与(2)相同但他汀类药物剂量加倍。此外,模拟了(针对性的)单独使用抗高血压和/或他汀类药物的情况。
主要结局指标 预防的急性心肌梗死或中风病例、获得的质量调整生命年(QALY)以及每获得一个QALY的成本。所有干预措施均与常规治疗进行比较。
结果 与常规治疗相比,所有方案均具有成本效益,每获得一个QALY的增量成本效益比在7900欧元至12300欧元之间。不含阿司匹林且含有双倍剂量他汀类药物的复方制剂获得的健康收益最大。以7.5%的10年风险为阈值,这种药丸可预防约3.5%的所有心血管事件。
结论 基于全球心血管风险评估的机会性筛查,随后为风险增加的人群开具复方制剂,提供了一种具有成本效益的策略。不含阿司匹林且他汀类药物剂量加倍的复方制剂获得的健康收益最大。