Department of Medicine, Columbia University Medical Center, New York, New York, USA.
Am J Cardiol. 2012 Apr 1;109(7):981-7. doi: 10.1016/j.amjcard.2011.11.027. Epub 2012 Jan 3.
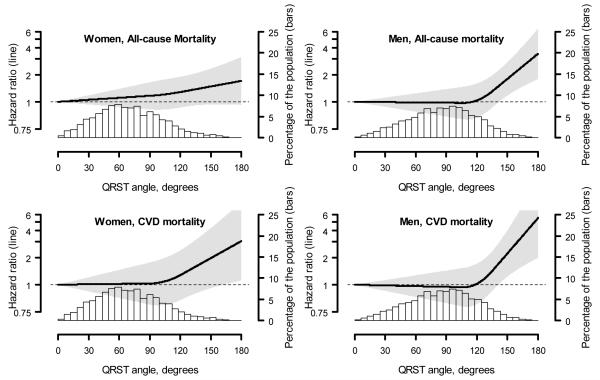
On the surface electrocardiogram, an abnormally wide QRS|T angle reflects changes in the regional action potential duration profiles and in the direction of the repolarization sequence, which is thought to increase the risk of ventricular arrhythmia. We investigated the relation between an abnormal QRS|T angle and mortality in a nationally representative sample of subjects without clinically evident heart disease. We studied 7,052 participants ≥40 years old in the third National Health and Nutrition Examination Survey with 12-lead electrocardiograms. Those with self-reported or electrocardiographic evidence of a previous myocardial infarction, QRS duration of ≥120 ms, or history of heart failure were excluded. Borderline and abnormal spatial QRS|T angles were defined according to gender-specific 75th and 95th percentiles of frequency distributions. All-cause (1,093 women and 1,191 men) and cardiovascular (462 women and 455 men) mortality during the 14-year period was assessed through linkage with the National Death Index. On multivariate analyses, an abnormal spatial QRS|T angle was associated with an increased hazard ratio (HR) for cardiovascular mortality in women (HR 1.82, 95% confidence interval 1.05 to 3.14) and men (HR 2.21, 95% confidence interval 1.32 to 3.68). Also, the multivariate adjusted HR for all-cause mortality associated with an abnormal QRS|T angle was 1.30 (95% confidence interval 0.95 to 1.78) for women and 1.87 (95% confidence interval 1.29 to 2.7) for men. A borderline QRS|T angle was not associated with an increased risk of all-cause or cardiovascular mortality. In conclusion, an abnormal QRS|T angle, as measured on a 12-lead electrocardiogram, was associated with an increased risk of cardiovascular and all-cause mortality in this population-based sample without known heart disease.
在体表心电图上,异常宽的 QRS|T 角反映了区域性动作电位时程谱和复极顺序方向的变化,这被认为会增加室性心律失常的风险。我们在一个没有明显临床心脏病的代表性全国性样本中调查了异常 QRS|T 角与死亡率之间的关系。我们研究了第三次国家健康和营养检查调查中 7052 名年龄在 40 岁及以上的 12 导联心电图参与者。排除了有先前心肌梗死、QRS 持续时间≥120ms 或心力衰竭病史的自我报告或心电图证据的患者。根据性别特异性频率分布的第 75 和 95 百分位数,定义了边缘和异常空间 QRS|T 角。通过与国家死亡指数的链接,评估了 14 年期间的全因(1093 名女性和 1191 名男性)和心血管(462 名女性和 455 名男性)死亡率。在多变量分析中,异常空间 QRS|T 角与女性(HR 1.82,95%置信区间 1.05 至 3.14)和男性(HR 2.21,95%置信区间 1.32 至 3.68)心血管死亡率的风险比(HR)增加相关。此外,与异常 QRS|T 角相关的全因死亡率的多变量校正 HR 为女性 1.30(95%置信区间 0.95 至 1.78),男性 1.87(95%置信区间 1.29 至 2.7)。边缘 QRS|T 角与全因或心血管死亡率的风险增加无关。总之,在这个没有已知心脏病的基于人群的样本中,12 导联心电图上测量的异常 QRS|T 角与心血管和全因死亡率的风险增加相关。