Normal Pressure Hydrocephalus Center, Otowa Hospital, Kyoto, Japan.
Fluids Barriers CNS. 2012 Jan 13;9(1):1. doi: 10.1186/2045-8118-9-1.
The cerebrospinal fluid (CSF) tap test (TT) has been regarded as an important test for the prediction of shunt effectiveness in patients with suspected idiopathic normal pressure hydrocephalus (iNPH). Although its specificity and sensitivity are reportedly high, there remains some disagreement over this point. Herein, the TT as a test for predicting shunt effectiveness was investigated in our multicenter prospective study named SINPHONI and strategies to increase its predictability were examined.
One hundred suspected iNPH patients with the following entry criteria were enrolled in the study: (1) 60 to 85 years old, (2) one or more of the NPH triad signs, (3) ventriculomegaly (Evans index > 0.3), (4) high convexity tightness in coronal-section MRI, and (5) no antecedent disorders. Changes in NPH triad symptoms were assessed using the iNPH grading scale and other measures before and after removal of 30 ml lumbar CSF. A positive response to TT was pre-defined by specific improvements on the grading and other scales. A ventriculoperitoneal shunt was performed with a programmable valve. The sensitivity and specificity of the TT was calculated with a contingency table. A decision tree analysis was performed to increase the predictability of the TT.
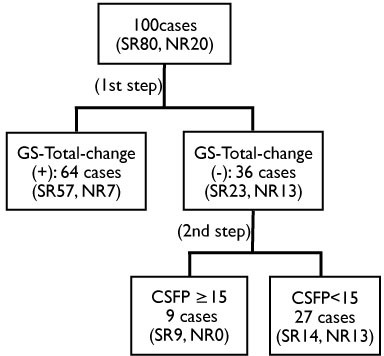
Among 100 patients, 80 were shunt responders. A statistically-significant variable between shunt responders and non-responders was CSF pressure. The changes in single variables in the iNPH grading scale after TT showed high specificity with low sensitivity. In contrast, change of the total score in the iNPH grading scale showed a relatively high sensitivity of 71.3% with specificity of 65%. A decision tree analysis revealed that using the iNPH grading scale total score and pre-shunt CSF pressure ≥ 15 cmH20, sensitivity increased to 82.5%, without a decrease in specificity.
The sensitivity and specificity of the TT for predicting shunt responsiveness were optimum when improvement on any iNPH grading scale was combined with CSF pressure ≥ 15 cmH20. To increase the sensitivity of the TT, further effort is necessary.
This study is registered with ClinicalTrials.gov, with the number NCT00221091.
脑脊液(CSF)穿刺试验(TT)已被认为是预测疑似特发性正常压力脑积水(iNPH)患者分流效果的重要检查。尽管其特异性和敏感性据称很高,但对此仍存在一些争议。在此,我们通过一项名为 SINPHONI 的多中心前瞻性研究,对 TT 作为预测分流效果的检查进行了研究,并探讨了提高其预测性的策略。
本研究共纳入 100 例符合以下纳入标准的疑似 iNPH 患者:(1)年龄 60-85 岁;(2)存在 NPH 三联征中的一项或多项;(3)脑室扩大(Evans 指数>0.3);(4)冠状位 MRI 显示脑凸面紧;(5)无既往疾病。在去除 30ml 腰穿脑脊液前后,使用 iNPH 分级量表和其他措施评估 NPH 三联征症状的变化。通过特定的分级和其他量表上的改善,将 TT 阳性定义为阳性反应。使用程控分流阀进行脑室-腹腔分流术。使用列联表计算 TT 的灵敏度和特异性。通过决策树分析来提高 TT 的预测性。
100 例患者中,80 例为分流有效者。分流有效者和无效者之间有统计学意义的变量是 CSF 压力。TT 后单个变量在 iNPH 分级量表中的变化具有高特异性和低灵敏度。相比之下,iNPH 分级量表总分的变化具有相对较高的灵敏度(71.3%)和特异性(65%)。决策树分析显示,使用 iNPH 分级量表总分和术前 CSF 压力≥15cmH20,灵敏度提高到 82.5%,特异性无下降。
当任何 iNPH 分级量表的改善与 CSF 压力≥15cmH20 相结合时,TT 预测分流反应的灵敏度和特异性最佳。为了提高 TT 的灵敏度,需要进一步努力。
本研究在 ClinicalTrials.gov 注册,编号为 NCT00221091。