Research Centre, Centre Hospitalier de l'Université de Montréal (CHUM) - Hôtel-Dieu, Montréal, H2W 1T7, Canada.
AIDS Res Ther. 2012 Feb 1;9:3. doi: 10.1186/1742-6405-9-3.
Several lines of evidence suggest that retinoids (retinol-ROL or vitamin A, and its active metabolites, retinoic acids-RAs) play important pathogenic roles in HIV infection and combination antiretroviral therapy (cART)-related events. We previously reported that antiretrovirals alter RAs synthesis in vitro. We hypothesised that in vivo serum retinoid concentrations are affected by both cART and HIV infection. This might explain several clinical and laboratory abnormalities reported in HIV-infected patients receiving cART.
The effects of optimal cART and chronic HIV on serum retinoids were firstly assessed longitudinally in 10 HIV-infected adults (group1 = G1): twice while on optimal cART (first, during long-term and second, during short term cART) and twice during 2 cART interruptions when HIV viral load (VL) was detectable. Retinoid concentrations during optimal long term cART in G1 were compared with cross-sectional results from 12 patients (G2) with suboptimal cART (detectable VL) and from 28 healthy adults (G3). Serum retinoids were measured by HPLC with ultraviolet detection. Retinoid concentrations were correlated with VL, CD4+ T- cell count and percentages, CD8+38+ fluorescence, triglycerides, cholesterol and C-peptide serum levels.
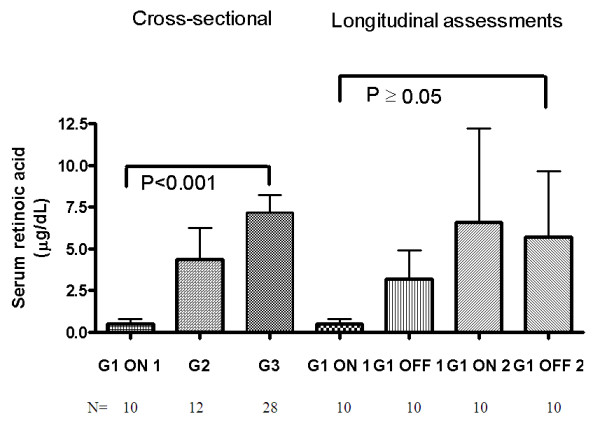
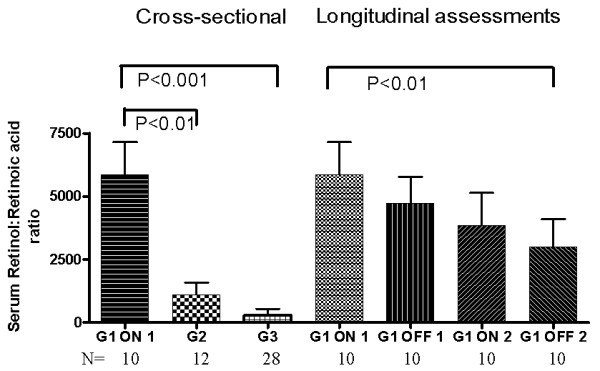
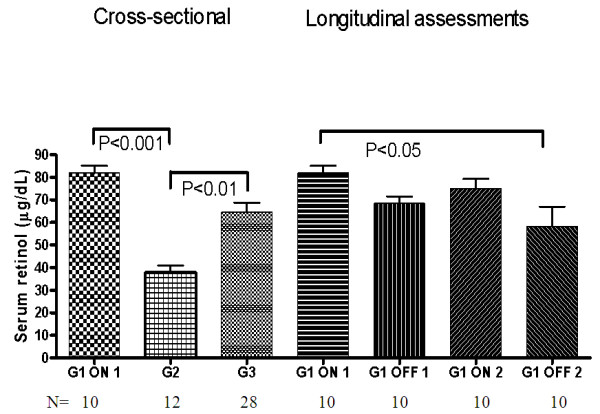
During optimal cART, G1 participants had drastically reduced RAs (0.5 ± 0.3 μg/dL; P < 0.01) but the highest ROL (82 ± 3.0 μg/dL) concentrations. During cART interruptions in these patients, RAs slightly increased whereas ROL levels diminished significantly (P < 0.05). G3 had the highest RAs levels (7.2 ± 1.1 μg/dL) and serum ROL comparable to values in North Americans. Serum ROL was decreased in G2 (37.7 ± 3.2 μg/dL; P < 0.01). No correlations were noted between RA and ROL levels or between retinoid concentrations and CD4+ T- cell count, CD8+38+ fluorescence, VL. ROL correlated with triglycerides and cholesterol in G1 (rs = 0.8; P = 0.01).
Serum RAs levels are significantly diminished by cART, whereas ROL concentrations significantly decreased during uncontrolled HIV infection but augmented with optimal cART. These alterations in retinoid concentrations may affect the expression of retinoid-responsive genes involved in metabolic, hormonal and immune processes and be responsible for some adverse events observed in HIV-infected persons treated with antiretrovirals. Further studies should assess concomitant serum and intracellular retinoid levels in different clinical situations in larger, homogenous populations.
有几条证据表明类视黄醇(视黄醇-ROL 或维生素 A 及其活性代谢产物维甲酸-RAs)在 HIV 感染和联合抗逆转录病毒治疗(cART)相关事件中发挥重要的致病作用。我们之前报道过抗逆转录病毒会改变体外 RAs 的合成。我们假设体内血清视黄醇浓度既受 cART 又受 HIV 感染的影响。这可能解释了在接受 cART 的 HIV 感染患者中报告的一些临床和实验室异常。
我们首先在 10 名 HIV 感染成人(G1 组)中纵向评估最佳 cART 和慢性 HIV 对血清视黄醇的影响:两次在最佳 cART 时(第一次在长期 cART 时,第二次在短期 cART 时)和两次在 HIV 病毒载量(VL)可检测时 cART 中断时。G1 中最佳长期 cART 时的视黄醇浓度与 12 名接受亚最佳 cART(可检测 VL)的患者(G2)和 28 名健康成年人(G3)的横截面结果进行了比较。采用 HPLC-UV 法检测血清视黄醇。视黄醇浓度与 VL、CD4+T 细胞计数和百分比、CD8+38+荧光、甘油三酯、胆固醇和 C 肽血清水平相关。
在最佳 cART 期间,G1 参与者的 RAs(0.5 ± 0.3 μg/dL;P < 0.01)明显降低,但 ROL(82 ± 3.0 μg/dL)浓度最高。在此类患者的 cART 中断期间,RA 略有增加,而 ROL 水平显著降低(P < 0.05)。G3 的 RAs 水平最高(7.2 ± 1.1 μg/dL),血清 ROL 与北美人相当。G2 的血清 ROL 降低(37.7 ± 3.2 μg/dL;P < 0.01)。RA 和 ROL 水平之间或视黄醇浓度与 CD4+T 细胞计数、CD8+38+荧光、VL 之间均无相关性。ROL 在 G1 中与甘油三酯和胆固醇相关(rs = 0.8;P = 0.01)。
cART 显著降低血清 RAs 水平,而 HIV 未控制时 ROL 浓度显著降低,但最佳 cART 时增加。这些视黄醇浓度的变化可能会影响参与代谢、激素和免疫过程的视黄醇反应基因的表达,并可能导致接受抗逆转录病毒治疗的 HIV 感染者中观察到的一些不良事件。应在更大、更同质的人群中评估不同临床情况下的血清和细胞内视黄醇水平。