Center for Applied Molecular Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA.
J Theor Biol. 2012 May 21;301:122-40. doi: 10.1016/j.jtbi.2012.02.002. Epub 2012 Feb 9.
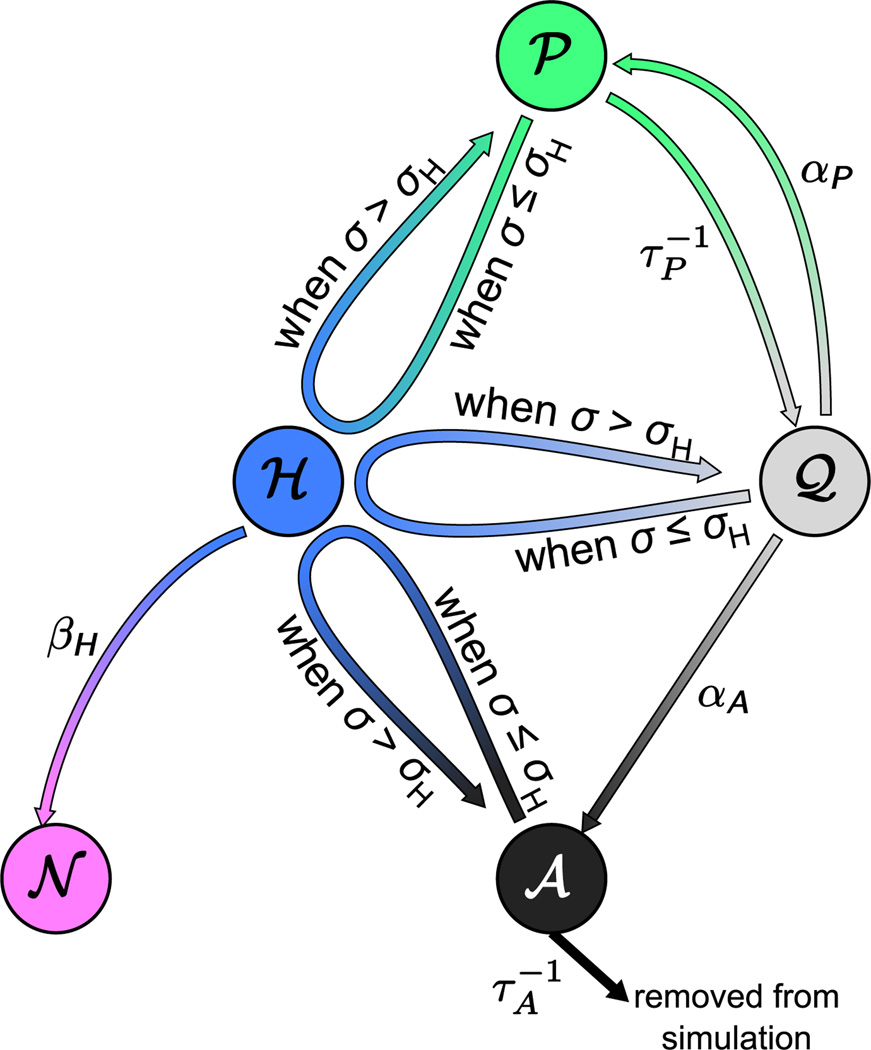
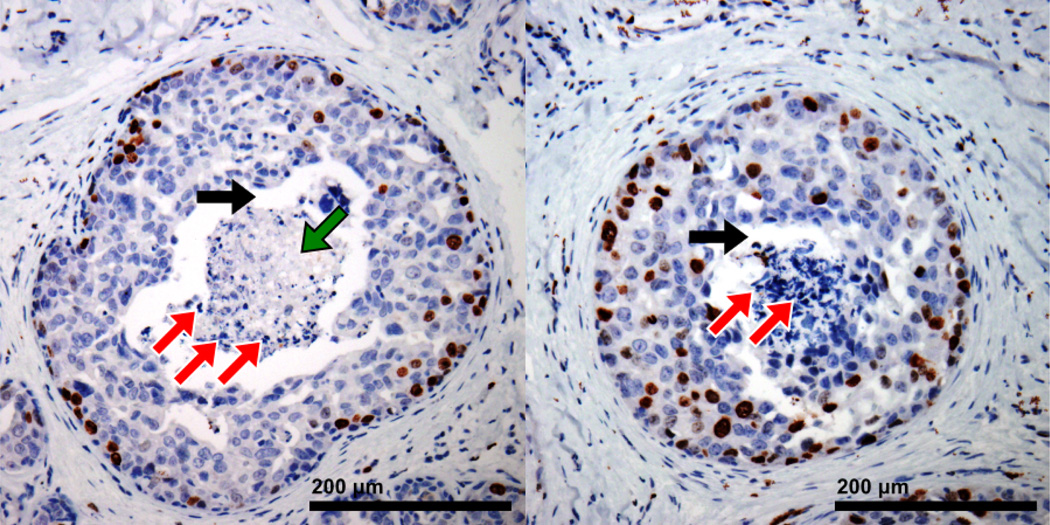
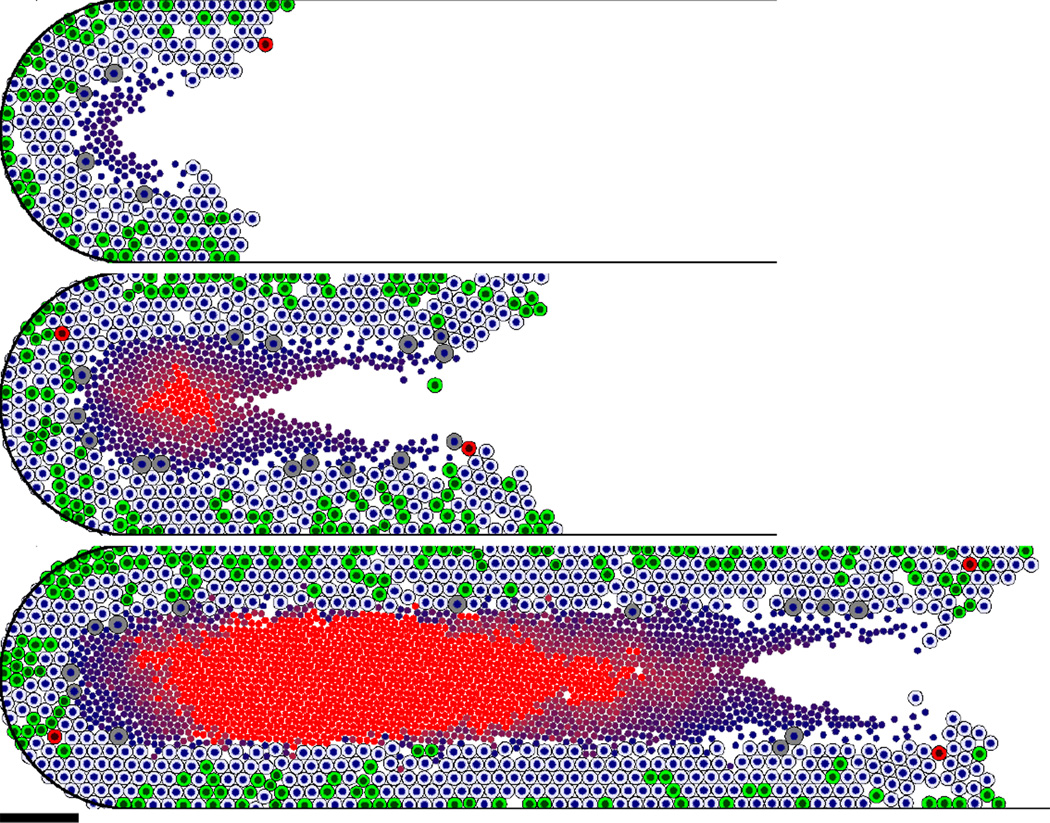
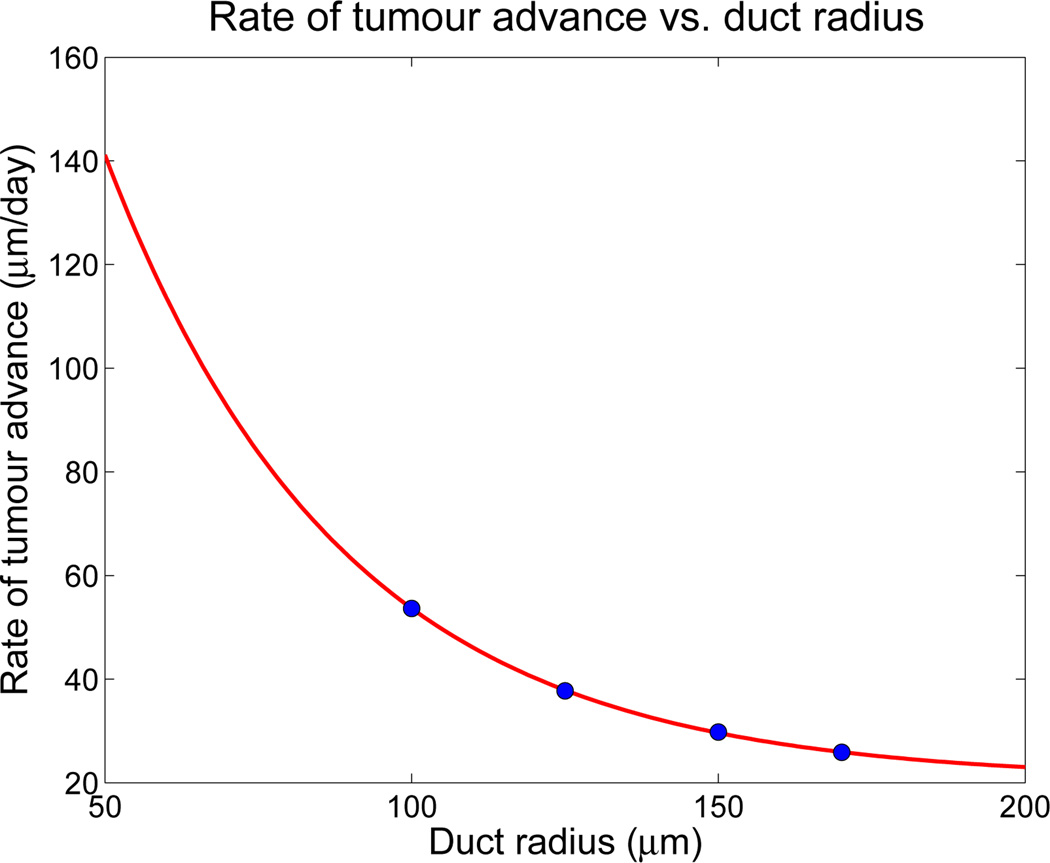
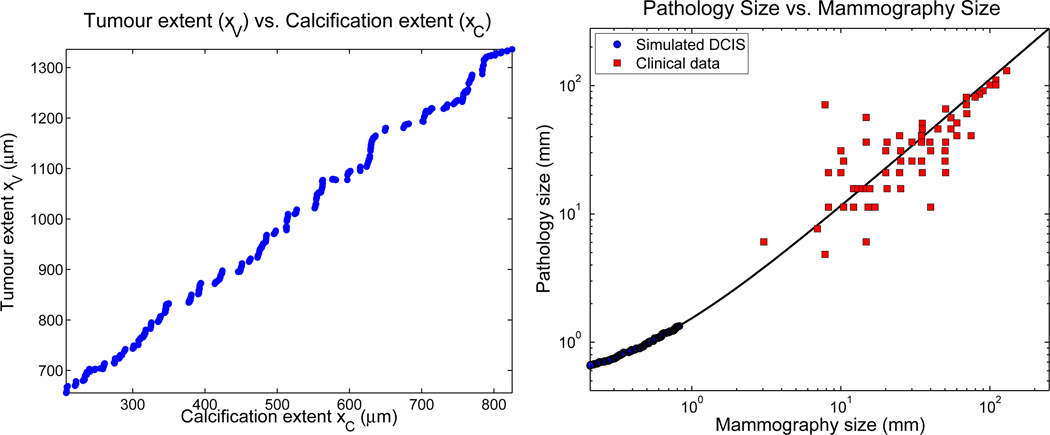
Ductal carcinoma in situ (DCIS)--a significant precursor to invasive breast cancer--is typically diagnosed as microcalcifications in mammograms. However, the effective use of mammograms and other patient data to plan treatment has been restricted by our limited understanding of DCIS growth and calcification. We develop a mechanistic, agent-based cell model and apply it to DCIS. Cell motion is determined by a balance of biomechanical forces. We use potential functions to model interactions with the basement membrane and amongst cells of unequal size and phenotype. Each cell's phenotype is determined by genomic/proteomic- and microenvironment-dependent stochastic processes. Detailed "sub-models" describe cell volume changes during proliferation and necrosis; we are the first to account for cell calcification. We introduce the first patient-specific calibration method to fully constrain the model based upon clinically-accessible histopathology data. After simulating 45 days of solid-type DCIS with comedonecrosis, the model predicts: necrotic cell lysis acts as a biomechanical stress relief and is responsible for the linear DCIS growth observed in mammography; the rate of DCIS advance varies with the duct radius; the tumour grows 7-10mm per year--consistent with mammographic data; and the mammographic and (post-operative) pathologic sizes are linearly correlated--in quantitative agreement with the clinical literature. Patient histopathology matches the predicted DCIS microstructure: an outer proliferative rim surrounds a stratified necrotic core with nuclear debris on its outer edge and calcification in the centre. This work illustrates that computational modelling can provide new insight on the biophysical underpinnings of cancer. It may 1-day be possible to augment a patient's mammography and other imaging with rigorously-calibrated models that help select optimal surgical margins based upon the patient's histopathologic data.
导管原位癌(DCIS)——一种显著的浸润性乳腺癌前体——通常在乳房 X 光片中被诊断为微钙化。然而,由于我们对 DCIS 生长和钙化的理解有限,乳房 X 光片和其他患者数据的有效利用一直受到限制。我们开发了一种基于机制的、基于代理的细胞模型,并将其应用于 DCIS。细胞运动由生物力学力的平衡决定。我们使用势函数来模拟与基底膜的相互作用以及大小和表型不等的细胞之间的相互作用。每个细胞的表型由基因组/蛋白质组和微环境依赖的随机过程决定。详细的“子模型”描述了细胞在增殖和坏死过程中的体积变化;我们是第一个考虑细胞钙化的。我们引入了第一个基于患者的校准方法,该方法基于临床可获得的组织病理学数据来完全约束模型。在模拟具有粉刺样坏死的实体型 DCIS 45 天后,该模型预测:坏死细胞裂解作为生物力学的应激缓解,负责在乳房 X 光片中观察到的线性 DCIS 生长;DCIS 进展的速度随导管半径而变化;肿瘤每年生长 7-10mm——与乳房 X 光数据一致;并且乳房 X 光和(术后)病理大小呈线性相关——与临床文献定量一致。患者组织病理学与预测的 DCIS 微观结构相匹配:增生性边缘环绕着分层坏死核心,其外边缘有核碎片,中心有钙化。这项工作表明,计算建模可以为癌症的生物物理基础提供新的见解。有朝一日,可能可以通过严格校准的模型来增强患者的乳房 X 光和其他成像,根据患者的组织病理学数据帮助选择最佳的手术边界。