Family AIDS Care and Education Services (FACES), Research Care and Training Program, Centre for Microbiology Research, Kenya Medical Research Institute, Kisumu, Kenya.
Department of Obstetrics, Gynecology and Reproductive Sciences, University of California San Francisco, San Francisco, CA, USA.
J Int AIDS Soc. 2012 Feb 22;15(1):8. doi: 10.1186/1758-2652-15-8.
Nyanza Province, Kenya, had the highest HIV prevalence in the country at 14.9% in 2007, more than twice the national HIV prevalence of 7.1%. Only 16% of HIV-infected adults in the country accurately knew their HIV status. Targeted strategies to reach and test individuals are urgently needed to curb the HIV epidemic. The family unit is one important portal.
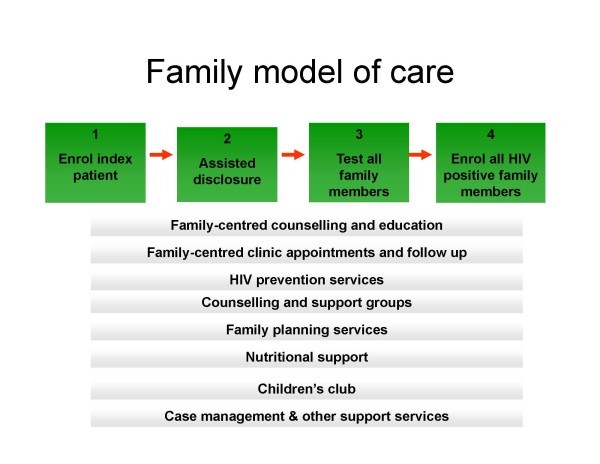
A family model of care was designed to build on the strengths of Kenyan families. Providers use a family information table (FIT) to guide index patients through the steps of identifying family members at HIV risk, address disclosure, facilitate family testing, and work to enrol HIV-positive members and to prevent new infections. Comprehensive family-centred clinical services are built around these steps. To assess the approach, a retrospective study of patients receiving HIV care between September 2007 and September 2009 at Lumumba Health Centre in Kisumu was conducted. A random sample of FITs was examined to assess family reach.
Through the family model of care, for each index patient, approximately 2.5 family members at risk were identified and 1.6 family members were tested. The approach was instrumental in reaching children; 61% of family members identified and tested were children. The approach also led to identifying and enrolling a high proportion of HIV- positive partners among those tested: 71% and 89%, respectively.
The family model of care is a feasible approach to broaden HIV case detection and service reach. The approach can be adapted for the local context and should continue to utilize index patient linkages, FIT adaption, and innovative methods to package services for families in a manner that builds on family support and enhances patient care and prevention efforts. Further efforts are needed to increase family member engagement.
肯尼亚的 Nyanza 省在 2007 年的艾滋病毒流行率最高,达到 14.9%,是全国艾滋病毒流行率 7.1%的两倍多。该国只有 16%的艾滋病毒感染者准确知晓自己的艾滋病毒状况。迫切需要采取有针对性的战略,接触和检测个人,以遏制艾滋病毒的流行。家庭是一个重要的切入点。
设计了一种家庭护理模式,以利用肯尼亚家庭的优势。提供者使用家庭信息表 (FIT) 来指导索引患者识别艾滋病毒风险的家庭成员,解决披露问题,促进家庭检测,并努力招募艾滋病毒阳性成员,防止新的感染。围绕这些步骤提供综合的以家庭为中心的临床服务。为了评估这种方法,对 2007 年 9 月至 2009 年 9 月期间在 Kisumu 的 Lumumba 保健中心接受艾滋病毒护理的患者进行了回顾性研究。对随机抽取的 FIT 进行了检查,以评估家庭的覆盖率。
通过家庭护理模式,每个索引患者平均识别和检测到 2.5 名有风险的家庭成员,检测到 1.6 名家庭成员。该方法在接触儿童方面发挥了重要作用;被识别和检测的家庭成员中,有 61%是儿童。该方法还导致在接受检测的人中发现和登记了很高比例的艾滋病毒阳性伴侣:分别为 71%和 89%。
家庭护理模式是扩大艾滋病毒病例发现和服务覆盖范围的可行方法。该方法可以根据当地情况进行调整,并应继续利用索引患者联系、FIT 适应和创新方法,以家庭支持为基础,为家庭打包服务,加强患者护理和预防工作。需要进一步努力提高家庭成员的参与度。