CIETcanada, 1 Stewart Street, Ottawa, Ontario, Canada.
BMC Health Serv Res. 2011 Dec 21;11 Suppl 2(Suppl 2):S5. doi: 10.1186/1472-6963-11-S2-S5.
After election in 1994, the South African government implemented national and regional programmes, such as the Wild Coast Spatial Development Initiative (SDI), to provoke economic growth and to decrease inequities. CIET measured development in the Wild Coast region across four linked cross-sectional surveys (1997-2007). The 2007 survey was an opportunity to look at inequities since the original 1997 baseline, and how such inequities affect access to health care.
The 2000, 2004 and 2007 follow-up surveys revisited the communities of the 1997 baseline. Household-level multivariate analysis looked at development indicators and access to health in the context of inequities such as household crowding, access to protected sources of water, house roof construction, main food item purchased, and perception of community empowerment. Individual multivariate models accounted for age, sex, education and income earning opportunities.
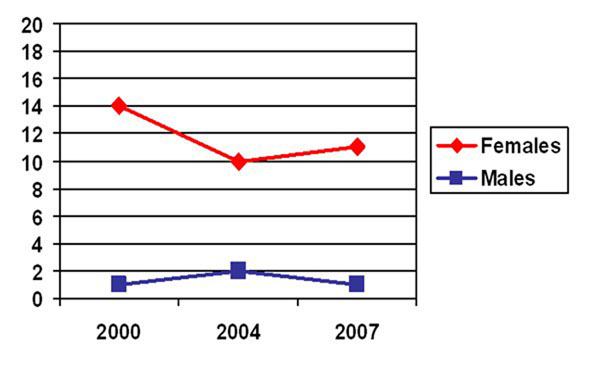
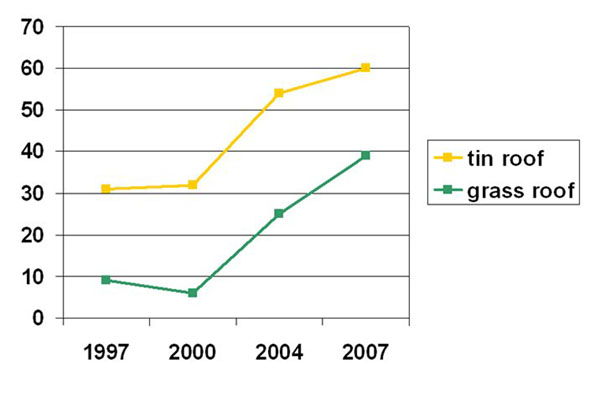
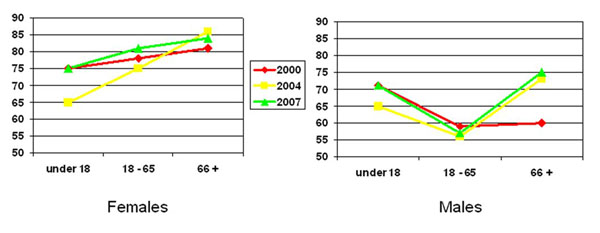
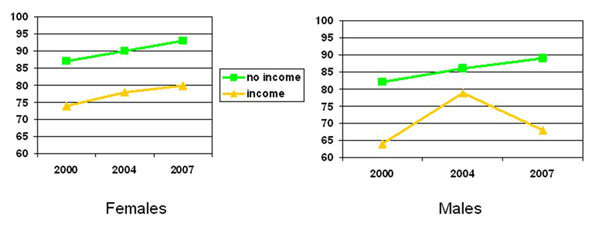
Overall access to protected sources of water increased since the baseline (from 20% in 1997 to 50% in 2007), yet households made of mud and grass, and households who bought basics as their main food item were still less likely to have protected sources of water. The most vulnerable, such as those with less education and less water and food security, were also less likely to have worked for wages leaving them with little chance of improving their standard of living (less education OR 0.59, 95%CI 0.37-0.94; less water security OR 0.67, 95%CI 0.48-0.93; less food security OR 0.43, 95%CI 0.29-0.64). People with less income were more likely to visit government services (among men OR 0.28, 95%CI 0.13-0.59; among women OR 0.33, 95%CI 0.20-0.54), reporting decision factors of cost and distance; users of private clinics sought out better service and medication. Lower food security and poorer house construction was also associated with women visiting government rather than private health services. Women with some formal education were nearly eight times more likely than women with no education to access health services for prevention rather than curative reasons (OR 7.65, 95%CI 4.10-14.25).
While there have been some improvements, the Wild Coast region still falls well below provincial and national standards in key areas such as access to clean water and employment despite years of government-led investment. Inequities remain prominent, particularly around access to health services.
1994 年选举后,南非政府实施了国家和地区计划,如野生海岸空间发展倡议(SDI),以促进经济增长和减少不平等。CIET 在四个相关的横断面调查(1997-2007 年)中衡量了野生海岸地区的发展。2007 年的调查是观察自最初 1997 年基线以来的不平等情况以及这种不平等如何影响获得医疗保健的机会的机会。
2000 年、2004 年和 2007 年的后续调查重新访问了 1997 年基线的社区。家庭层面的多变量分析着眼于发展指标和在家庭拥挤、获得受保护水源、房屋屋顶建设、主要购买的食物以及社区赋权感知等不平等方面获得医疗保健。个体多变量模型考虑了年龄、性别、教育和收入机会。
自基线以来,获得受保护水源的总体机会增加(从 1997 年的 20%增加到 2007 年的 50%),但由泥土和草制成的家庭以及购买基本食物作为主要食物的家庭获得保护水源的可能性仍然较低。最脆弱的人群,如教育程度较低、水和粮食安全程度较低的人群,获得工资的可能性也较小,从而几乎没有机会改善生活水平(受教育程度较低或 0.59,95%CI 0.37-0.94;水安全程度较低或 0.67,95%CI 0.48-0.93;粮食安全程度较低或 0.43,95%CI 0.29-0.64)。收入较低的人更有可能访问政府服务(男性或 0.28,95%CI 0.13-0.59;女性或 0.33,95%CI 0.20-0.54),报告成本和距离的决策因素;使用私人诊所的人寻求更好的服务和药物。较低的粮食安全和较差的房屋建设也与妇女前往政府而不是私人保健服务有关。接受过一些正规教育的妇女比没有接受过教育的妇女更有可能出于预防而不是治疗原因获得保健服务(OR 7.65,95%CI 4.10-14.25)。
尽管多年来政府主导的投资,但野生海岸地区在获得清洁水和就业等关键领域仍远低于省级和国家标准,尽管取得了一些进展。不平等现象仍然突出,特别是在获得保健服务方面。