Ipas India, Vasant Vihar, New Delhi, India.
BMC Public Health. 2012 Mar 9;12:175. doi: 10.1186/1471-2458-12-175.
Unsafe abortion in India leads to significant morbidity and mortality. Abortion has been legal in India since 1971, and the availability of safe abortion services has increased. However, service availability has not led to a significant reduction in unsafe abortion. This study aimed to understand the gap between safe abortion availability and use of services in Bihar and Jharkhand, India by examining accessibility from the perspective of rural, Indian women.
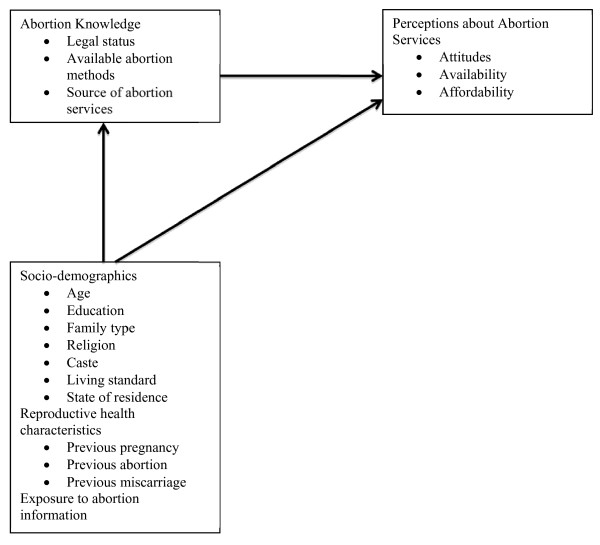
Two-stage stratified random sampling was used to identify and enroll 1411 married women of reproductive age in four rural districts in Bihar and Jharkhand, India. Data were collected on women's socio-demographic characteristics; exposure to mass media and other information sources; and abortion-related knowledge, perceptions and practices. Multiple linear regression models were used to explore the association between knowledge and perceptions about abortion.
Most women were poor, had never attended school, and had limited exposure to mass media. Instead, they relied on community health workers, family and friends for health information. Women who had knowledge about abortion, such as knowing an abortion method, were more likely to perceive that services are available (β = 0.079; p < 0.05) and have positive attitudes toward abortion (β = 0.070; p < 0.05). In addition, women who reported exposure to abortion messages were more likely to have favorable attitudes toward abortion (β = 0.182; p < 0.05).
Behavior change communication (BCC) interventions, which address negative perceptions by improving community knowledge about abortion and support local availability of safe abortion services, are needed to increase enabling resources for women and improve potential access to services. Implementing BCC interventions is challenging in settings such as Bihar and Jharkhand where women may be difficult to reach directly, but interventions can target individuals in the community to transfer information to the women who need this information most. Interpersonal approaches that engage community leaders and influencers may also counteract negative social norms regarding abortion and associated stigma. Collaborative actions of government, NGOs and private partners should capitalize on this potential power of communities to reduce the impact of unsafe abortion on rural women.
印度不安全堕胎导致了严重的发病率和死亡率。自 1971 年以来,印度的堕胎合法化,安全堕胎服务的可及性有所增加。然而,服务的可及性并没有导致不安全堕胎的显著减少。本研究旨在通过考察农村印度妇女的可及性,了解印度比哈尔邦和恰尔康德邦安全堕胎服务的提供与使用之间的差距。
采用两阶段分层随机抽样的方法,在印度比哈尔邦和恰尔康德邦的四个农村地区,共确定并招募了 1411 名已婚育龄妇女。收集了妇女的社会人口特征;接触大众媒体和其他信息来源;以及与堕胎相关的知识、看法和做法。采用多元线性回归模型来探讨关于堕胎的知识与看法之间的关系。
大多数妇女都很贫穷,从未上过学,很少接触大众媒体。相反,她们依靠社区卫生工作者、家庭和朋友获取健康信息。对堕胎有了解的妇女,如知道堕胎方法,更有可能认为服务是可获得的(β=0.079;p<0.05),对堕胎有积极的态度(β=0.070;p<0.05)。此外,报告接触过堕胎信息的妇女更有可能对堕胎持赞成态度(β=0.182;p<0.05)。
需要实施行为改变沟通(BCC)干预措施,通过提高社区对堕胎的了解,支持当地安全堕胎服务的提供,来消除负面看法,为妇女提供更多的有利资源,并改善获得服务的潜力。在比哈尔邦和恰尔康德邦等妇女难以直接接触的环境中,实施 BCC 干预措施具有挑战性,但可以针对社区中的个人,将信息传递给最需要这些信息的妇女。利用社区领袖和有影响力者的人际方法也可以抵制与堕胎相关的负面社会规范和污名化。政府、非政府组织和私营部门合作伙伴应共同努力,利用社区的这一潜在力量,减少不安全堕胎对农村妇女的影响。