The Kirby Institute, University of New South Wales, Sydney, NSW 2052, Australia.
BMC Public Health. 2012 Mar 23;12:234. doi: 10.1186/1471-2458-12-234.
Antiretroviral therapy (ART) has substantially decreased mortality and HIV-related morbidity. However, other morbidities appear to be more common among PLHIV than in the general population. This study aimed to estimate the relative risk of renal disease among people living with HIV (PLHIV) compared to the HIV-uninfected population.
We conducted a systematic review and meta-analysis of relative risks of renal disease among populations of PLHIV reported in studies from the peer-reviewed literature. We searched Medline for relevant journal articles published before September 2010, yielding papers published during or after 2002. We also searched conference proceedings of the International AIDS Society (IAS) and Conference on Retroviruses and Opportunistic Infections (CROI) prior to and including 2010. Eligible studies were observational studies reporting renal disease defined as acute or chronic reduced renal function with glomerular filtration rate less than or equal to 60 ml/min/1.73 m2 among HIV-positive adults. Pooled relative risks were calculated for various groupings, including class of ART drugs administered.
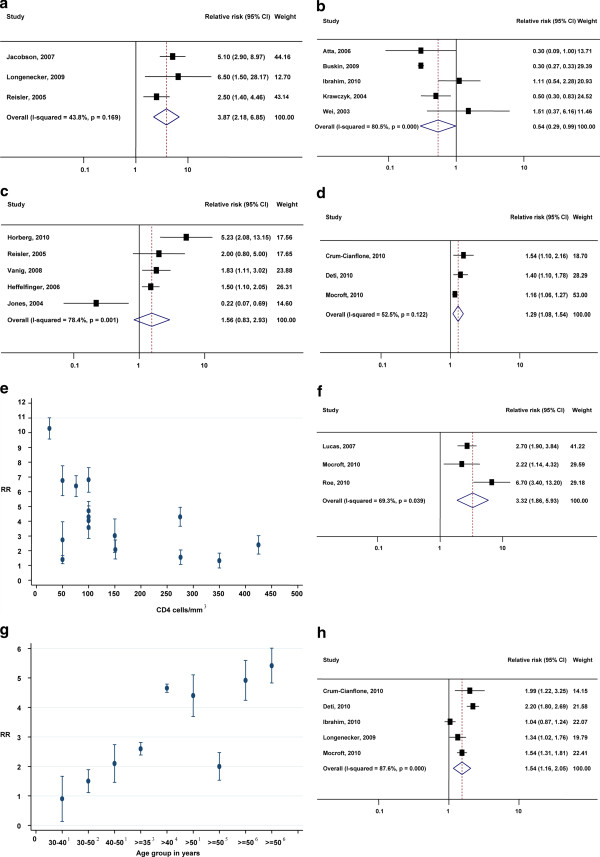
The overall relative risk of renal disease was 3.87 (95% CI: 2.85-6.85) among HIV-infected people compared to HIV-uninfected people. The relative risk of renal disease among people with late-stage HIV infection (AIDS) was 3.32 (1.86-5.93) compared to other PLHIV. The relative risk of renal disease among PLHIV who were receiving antiretroviral therapy (ART) was 0.54 (0.29-0.99) compared to treatment-naïve PLHIV; the relative risk of renal disease among PLHIV who were treated with tenofovir was 1.56 (0.83-2.93) compared to PLHIV who were treated with non-tenofovir therapy. The risk of renal disease was also found to significantly increase with age.
PLHIV are at increased risk of renal disease, with greater risk at later stages of infection and at older ages. ART prolongs survival and decreases the risk of renal disease. However, less reduction in renal disease risk occurs for Tenofovir-containing ART than for other regimens.
抗逆转录病毒疗法(ART)大大降低了死亡率和与 HIV 相关的发病率。然而,其他疾病在 HIV 感染者(PLHIV)中的发病率似乎高于普通人群。本研究旨在评估与未感染 HIV 的人群相比,PLHIV 发生肾脏疾病的相对风险。
我们对从同行评议文献中报告的 PLHIV 人群研究中肾脏疾病的相对风险进行了系统评价和荟萃分析。我们在 Medline 中搜索了截至 2010 年 9 月之前发表的相关期刊文章,得到了 2002 年及以后发表的文章。我们还搜索了国际艾滋病协会(IAS)和逆转录病毒和机会性感染会议(CROI)的会议记录,包括 2010 年及以前的记录。合格的研究为观察性研究,报告了肾脏疾病定义为肾小球滤过率(GFR)小于或等于 60ml/min/1.73m2 的急性或慢性肾功能降低,包括 HIV 阳性成年人。计算了各种分组的汇总相对风险,包括给予的 ART 药物类别。
与未感染 HIV 的人群相比,HIV 感染者患肾脏疾病的总体相对风险为 3.87(95%CI:2.85-6.85)。晚期 HIV 感染(艾滋病)患者患肾脏疾病的相对风险为 3.32(1.86-5.93),与其他 PLHIV 相比。与未接受抗逆转录病毒治疗(ART)的 PLHIV 相比,接受 ART 治疗的 PLHIV 发生肾脏疾病的相对风险为 0.54(0.29-0.99);与接受非替诺福韦治疗的 PLHIV 相比,接受替诺福韦治疗的 PLHIV 发生肾脏疾病的相对风险为 1.56(0.83-2.93)。研究还发现,肾脏疾病的风险随着年龄的增长而显著增加。
PLHIV 患肾脏疾病的风险增加,感染后期和年龄较大时风险更高。ART 可延长生存期并降低肾脏疾病的风险。然而,替诺福韦包含的 ART 方案比其他方案降低肾脏疾病风险的效果较小。