Tayside Medicines Unit, NHS Tayside, Mackenzie Building, Kirsty Semple Way, Dundee DD2 4BF, UK.
Implement Sci. 2012 Mar 23;7:24. doi: 10.1186/1748-5908-7-24.
High-risk prescribing of non-steroidal anti-inflammatory drugs (NSAIDs) and antiplatelet agents accounts for a significant proportion of hospital admissions due to preventable adverse drug events. The recently completed PINCER trial has demonstrated that a one-off pharmacist-led information technology (IT)-based intervention can significantly reduce high-risk prescribing in primary care, but there is evidence that effects decrease over time and employing additional pharmacists to facilitate change may not be sustainable.
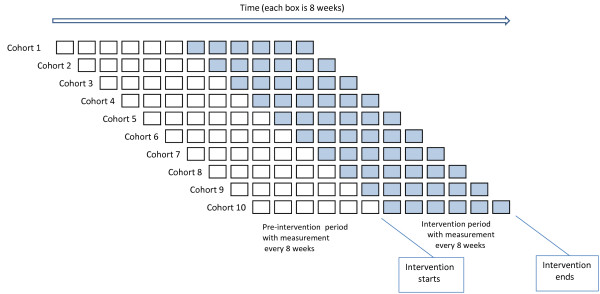
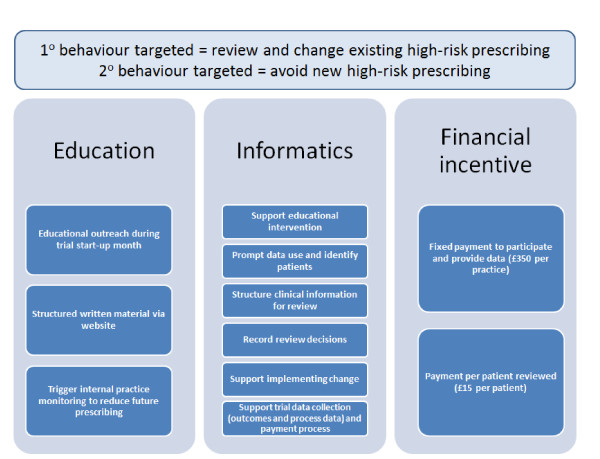
METHODS/DESIGN: We will conduct a cluster randomised controlled with a stepped wedge design in 40 volunteer general practices in two Scottish health boards. Eligible practices are those that are using the INPS Vision clinical IT system, and have agreed to have relevant medication-related data to be automatically extracted from their electronic medical records. All practices (clusters) that agree to take part will receive the data-driven quality improvement in primary care (DQIP) intervention, but will be randomised to one of 10 start dates. The DQIP intervention has three components: a web-based informatics tool that provides weekly updated feedback of targeted prescribing at practice level, prompts the review of individual patients affected, and summarises each patient's relevant risk factors and prescribing; an outreach visit providing education on targeted prescribing and training in the use of the informatics tool; and a fixed payment of 350 GBP (560 USD; 403 EUR) up front and a small payment of 15 GBP (24 USD; 17 EUR) for each patient reviewed in the 12 months of the intervention. We hypothesise that the DQIP intervention will reduce a composite of nine previously validated measures of high-risk prescribing. Due to the nature of the intervention, it is not possible to blind practices, the core research team, or the data analyst. However, outcome assessment is entirely objective and automated. There will additionally be a process and economic evaluation alongside the main trial.
The DQIP intervention is an example of a potentially sustainable safety improvement intervention that builds on the existing National Health Service IT-infrastructure to facilitate systematic management of high-risk prescribing by existing practice staff. Although the focus in this trial is on Non-steroidal anti-inflammatory drugs and antiplatelets, we anticipate that the tested intervention would be generalisable to other types of prescribing if shown to be effective.
ClinicalTrials.gov, dossier number: NCT01425502.
非甾体抗炎药(NSAIDs)和抗血小板药物的高危处方占因可预防药物不良事件而住院的重要比例。最近完成的 PINCER 试验表明,一次性药剂师主导的基于信息技术(IT)的干预可以显著减少初级保健中的高危处方,但有证据表明,效果会随着时间的推移而降低,并且雇用额外的药剂师来促进变革可能是不可持续的。
方法/设计:我们将在苏格兰两个卫生委员会的 40 家志愿全科诊所中进行一项以阶梯式楔形设计为基础的集群随机对照试验。符合条件的诊所是那些正在使用 INPS Vision 临床 IT 系统的诊所,并且同意从他们的电子病历中自动提取相关药物相关数据。所有同意参与的诊所(集群)都将接受初级保健中的数据驱动质量改进(DQIP)干预,但将随机分配到 10 个开始日期之一。DQIP 干预有三个组成部分:一个基于网络的信息工具,每周为实践水平提供有针对性的处方反馈,提示审查受影响的个别患者,并总结每位患者的相关风险因素和处方;一次外展访问,提供有针对性的处方教育和信息工具使用培训;以及一次性支付 350 英镑(560 美元;403 欧元),干预 12 个月内每审查一名患者支付 15 英镑(24 美元;17 欧元)。我们假设 DQIP 干预将降低以前验证的九项高危处方综合指标。由于干预的性质,无法对实践、核心研究团队或数据分析师进行盲法处理。但是,结果评估完全是客观和自动化的。除了主要试验之外,还将进行过程和经济评估。
DQIP 干预是一种潜在可持续的安全改进干预措施的示例,它利用现有的国家卫生服务 IT 基础设施来促进现有实践人员对高危处方的系统管理。尽管本试验的重点是非甾体抗炎药和抗血小板药物,但如果证明有效,我们预计经过测试的干预措施将适用于其他类型的处方。
ClinicalTrials.gov,注册编号:NCT01425502。