Department of Gastroenterology, Hepatology and Pathobiology, Lerner Research Institute, Cleveland Clinic, NE4-208, 9500 Euclid Avenue, Cleveland, OH, 44195, USA,
J Cachexia Sarcopenia Muscle. 2012 Dec;3(4):225-37. doi: 10.1007/s13539-012-0069-3. Epub 2012 May 31.
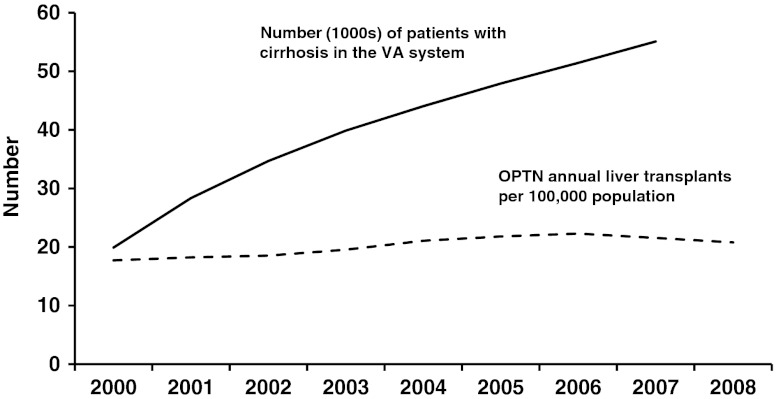
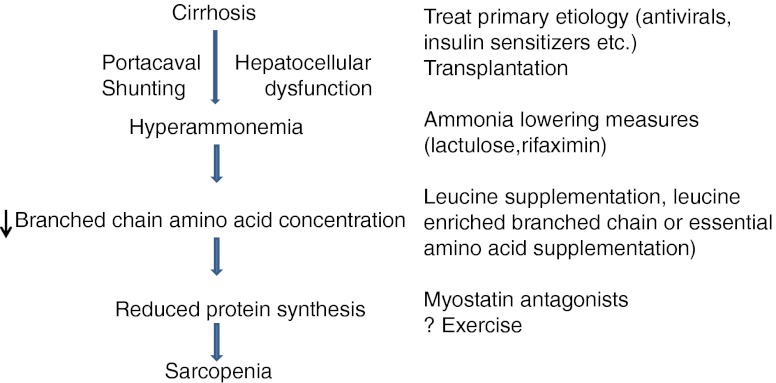
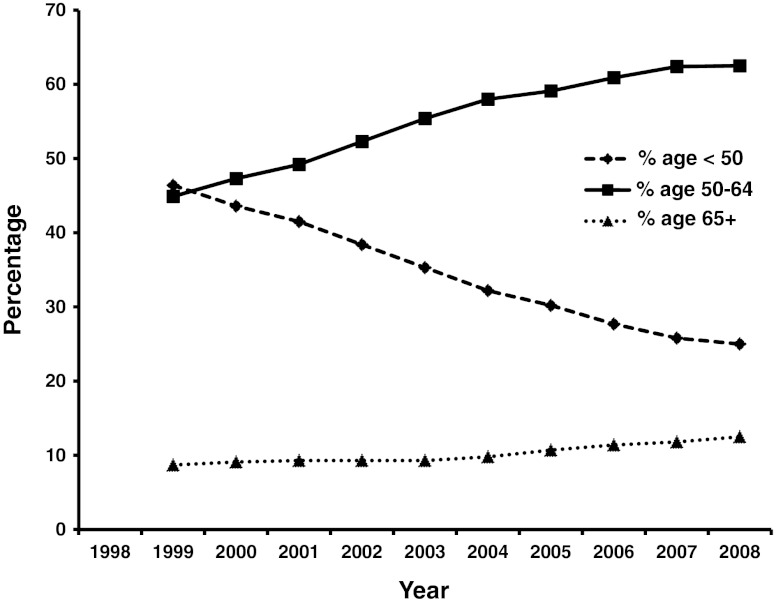
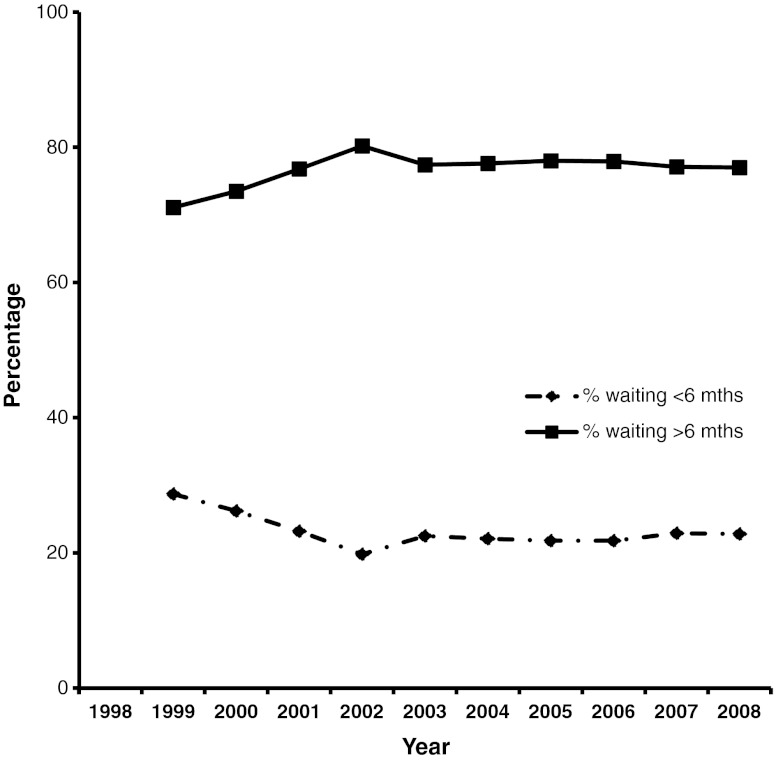
Cirrhosis is the consequence of progression of many forms of necro-inflammatory disorders of the liver with hepatic fibrosis, hepatocellular dysfunction, and vascular remodeling. Reversing the primary hepatic disorder, liver transplantation, and controlling the complications are the major management goals. Since the former options are not available to the majority of cirrhotics, treating complications remains the mainstay of therapy. Sarcopenia and/or cachexia is the most common complication and adversely affects survival, quality of life, development of other complications of cirrhosis, and outcome after liver transplantation. With the increase in number of cirrhotic patients with hepatitis C and nonalcoholic fatty liver disease, the number of patients waiting for a liver transplantation is likely to continue to increase above the currently estimated 72.3/100,000 population. One of the critical clinical questions is to determine if we can treat sarcopenia of cirrhosis without transplantation. No effective therapies exist to treat sarcopenia because the mechanism(s) of sarcopenia in cirrhosis is as yet unknown. The reasons for this include the predominantly descriptive studies to date and the advances in our understanding of skeletal muscle biology and molecular regulation of atrophy and hypertrophy not being translated into the clinical practice of hepatology. Satellite cell biology, muscle autophagy and apoptosis, and molecular signaling abnormalities in the skeletal muscle of cirrhotics are also not known. Aging of the cirrhotic and transplanted population, use of mTOR inhibitors, and the lack of definitive outcome measures to define sarcopenia and cachexia in this population add to the difficulty in increasing our understanding of hepatic sarcopenia/cachexia and developing treatment options. Recent data on the role of myostatin, AMP kinase, impaired mTOR signaling resulting in anabolic resistance in animal models, and the rapidly developing field of nutriceuticals as signaling molecules need to be evaluated in human cirrhotics. Finally, the benefits of exercise reported in other disease states with sarcopenia may not be safe in cirrhotics due to the risk of gastrointestinal variceal bleeding due to an increase in portal pressure. This article focuses on the problems facing both muscle biologists and hepatologists in developing a comprehensive approach to sarcopenia in cirrhosis.
肝硬化是肝脏发生多种坏死性炎症性疾病的后果,这些疾病伴有肝纤维化、肝细胞功能障碍和血管重构。逆转原发性肝疾病、进行肝移植和控制并发症是主要的治疗目标。由于大多数肝硬化患者无法选择前两种方案,因此治疗并发症仍然是治疗的主要手段。肌肉减少症和/或恶病质是最常见的并发症,会对生存率、生活质量、肝硬化其他并发症的发展以及肝移植后的结果产生不利影响。随着丙型肝炎和非酒精性脂肪性肝病肝硬化患者数量的增加,等待肝移植的患者数量可能会继续增加,超过目前估计的 72.3/10 万人口。一个关键的临床问题是确定我们是否可以在不进行移植的情况下治疗肝硬化性肌肉减少症。目前尚无有效的治疗方法可以治疗肝硬化性肌肉减少症,因为导致肝硬化性肌肉减少症的机制尚不清楚。造成这种情况的原因包括迄今为止主要是描述性研究,以及我们对骨骼肌生物学和萎缩和肥大的分子调节的理解的进步尚未转化为肝病学的临床实践。还不知道肝硬化患者骨骼肌中的卫星细胞生物学、肌肉自噬和细胞凋亡以及分子信号异常。肝硬化和移植人群的老龄化、使用 mTOR 抑制剂以及缺乏明确的结局测量标准来定义该人群中的肌肉减少症和恶病质,这也增加了增加我们对肝性肌肉减少症/恶病质的理解和开发治疗方案的难度。最近关于肌肉生长抑制素、AMP 激酶、mTOR 信号受损导致合成代谢抵抗在动物模型中的作用以及作为信号分子的营养保健品快速发展的研究数据需要在人类肝硬化患者中进行评估。最后,由于门静脉压力增加导致胃肠道静脉曲张出血的风险,在其他伴有肌肉减少症的疾病中报告的运动益处可能对肝硬化患者不安全。本文重点讨论了肌肉生物学家和肝病学家在制定肝硬化性肌肉减少症综合治疗方法方面面临的问题。