Independent Computer Scientist, P.O. Box 847, Pearblossom, CA 93553, United States.
Vaccine. 2013 Mar 25;31(13):1680-94. doi: 10.1016/j.vaccine.2012.05.050. Epub 2012 Jun 1.
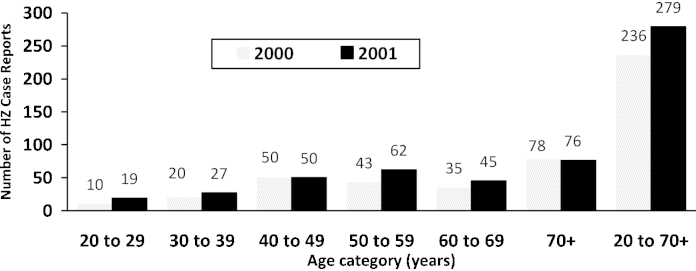
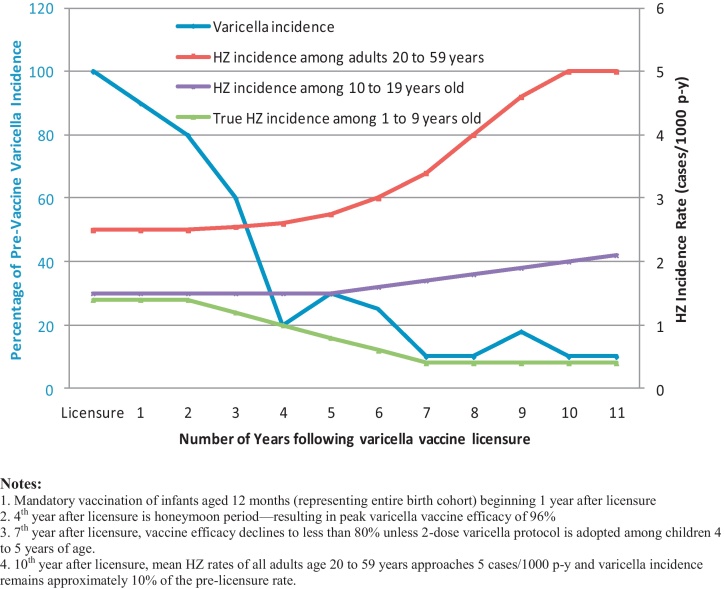
In a cooperative agreement starting January 1995, prior to the FDA's licensure of the varicella vaccine on March 17, the Centers for Disease Control and Prevention (CDC) funded the Los Angeles Department of Health Services' Antelope Valley Varicella Active Surveillance Project (AV-VASP). Since only varicella case reports were gathered, baseline incidence data for herpes zoster (HZ) or shingles was lacking. Varicella case reports decreased 72%, from 2834 in 1995 to 836 in 2000 at which time approximately 50% of children under 10 years of age had been vaccinated. Starting in 2000, HZ surveillance was added to the project. By 2002, notable increases in HZ incidence rates were reported among both children and adults with a prior history of natural varicella. However, CDC authorities still claimed that no increase in HZ had occurred in any US surveillance site. The basic assumptions inherent to the varicella cost-benefit analysis ignored the significance of exogenous boosting caused by those shedding wild-type VZV. Also ignored was the morbidity associated with even rare serious events following varicella vaccination as well as the morbidity from increasing cases of HZ among adults. Vaccine efficacy declined below 80% in 2001. By 2006, because 20% of vaccinees were experiencing breakthrough varicella and vaccine-induced protection was waning, the CDC recommended a booster dose for children and, in 2007, a shingles vaccination was approved for adults aged 60 years and older. In the prelicensure era, 95% of adults experienced natural chickenpox (usually as children)-these cases were usually benign and resulted in long-term immunity. Varicella vaccination is less effective than the natural immunity that existed in prevaccine communities. Universal varicella vaccination has not proven to be cost-effective as increased HZ morbidity has disproportionately offset cost savings associated with reductions in varicella disease. Universal varicella vaccination has failed to provide long-term protection from VZV disease.
在一项始于 1995 年 1 月的合作协议中,在 FDA 于 3 月 17 日批准水痘疫苗之前,疾病控制与预防中心(CDC)为洛杉矶卫生服务部的羚羊谷水痘主动监测项目(AV-VASP)提供了资金。由于只收集了水痘病例报告,因此缺乏带状疱疹(HZ)或带状疱疹的数据。自 2000 年开始,该项目增加了 HZ 监测。到 2002 年,有既往自然水痘史的儿童和成人的 HZ 发病率报告显著增加。然而,CDC 当局仍声称,在美国任何监测点都没有发生 HZ 增加。水痘成本效益分析中固有的基本假设忽略了由野生型 VZV 引发的外源性增强的重要性。也忽略了水痘疫苗接种后即使是罕见的严重事件相关的发病率以及成年人中 HZ 病例增加相关的发病率。疫苗效力在 2001 年下降到 80%以下。到 2006 年,由于 20%的疫苗接种者出现突破性水痘,疫苗诱导的保护作用减弱,CDC 建议为儿童接种加强针,2007 年,批准为 60 岁及以上的成年人接种带状疱疹疫苗。在许可前时代,95%的成年人经历过自然水痘(通常是在儿童时期)-这些病例通常是良性的,并产生长期免疫力。水痘疫苗接种的效果不如疫苗前社区中存在的自然免疫力。普遍水痘疫苗接种并不能证明具有成本效益,因为 HZ 发病率的增加不成比例地抵消了水痘疾病减少相关的成本节约。普遍水痘疫苗接种未能提供针对 VZV 疾病的长期保护。