Khutia Samit Kumar, Mandal Mohan C, Das Sabyasachi, Basu S R
Department of Anaesthesiology, North Bengal Medical College, P.O. Sushrutanagar, Darjeeling, West Bengal, India.
Indian J Anaesth. 2012 Mar;56(2):145-50. doi: 10.4103/0019-5049.96313.
Paediatric patients often present with different painful conditions that require immediate surgical interventions. Despite a plethora of articles on the ketamine-propofol combination, comprehensive evidence regarding the suitable sedoanalgesia regime is lacking due to heterogeneity in study designs.
This prospective, randomized, double-blind, active-controlled trial was conducted in 100 children, of age 3-14 years, American Society of Anesthesiologist physical status IE-IIE, posted for emergency short surgical procedures. Patients were randomly allocated to receive either 2 mL of normal saline (pre-induction) plus calculated volume of drug from the 11 mL of ketamine-propofol solution for induction (group PK, n=50) or fentanyl 1.5 μg/kg diluted to 2 mL with normal saline (pre-induction) plus calculated volume of drug from the 11 mL of propofol solution for induction (group PF, n=50). In both the groups, the initial bolus propofol 1 mg/kg i.v. (assuming the syringes contained only propofol, for simplicity) was followed by adjusted infusion to achieve a Ramsay Sedation Scale score of six. Mean arterial pressure (MAP) was the primary outcome measurement.
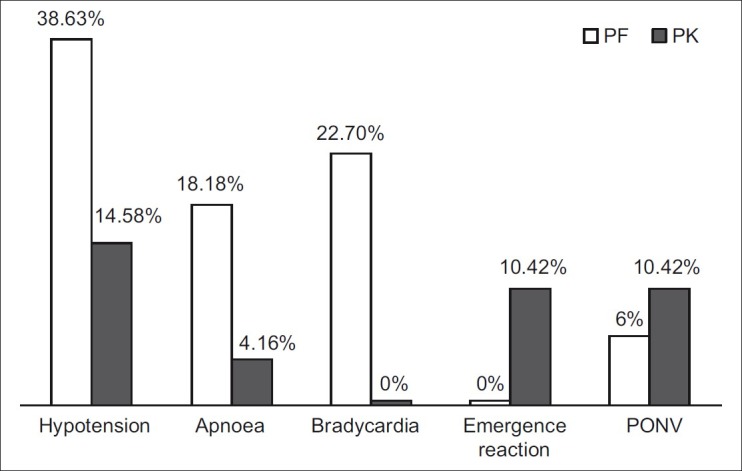
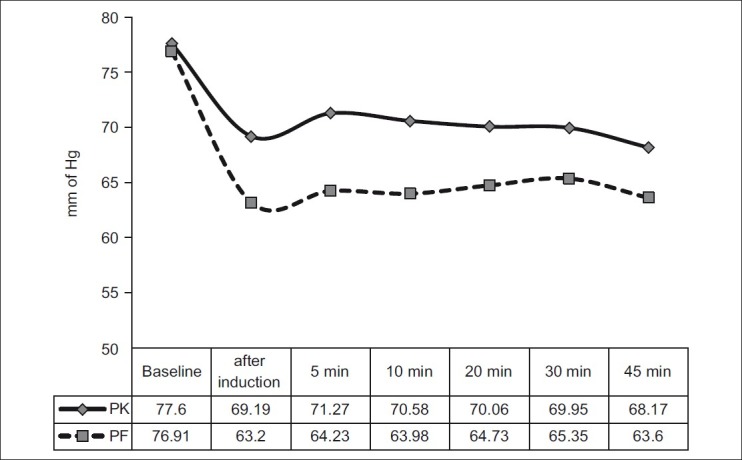
Data from 48 patients in group PK and 44 patients in group PF were available for analysis. Hypotension was found in seven patients (14.6%) in group PK compared with 17 (38.6%) patients in group PF (P=0.009). Intraoperative MAP was significantly lower in group PF than group PK when compared with baseline.
The combination of low-dose ketamine and propofol is more effective and a safer sedoanalgesia regimen than the propofol-fentanyl combination in paediatric emergency short surgical procedures in terms of haemodynamic stability and lesser incidence of apnoea.
儿科患者常出现需要立即进行手术干预的各种疼痛状况。尽管有大量关于氯胺酮 - 丙泊酚联合使用的文章,但由于研究设计的异质性,缺乏关于合适的镇静镇痛方案的全面证据。
本前瞻性、随机、双盲、活性对照试验纳入了100名年龄在3至14岁、美国麻醉医师协会身体状况分级为I - IIE级、需进行急诊短时间外科手术的儿童。患者被随机分配接受以下两种方案之一:2 mL生理盐水(诱导前)加从11 mL氯胺酮 - 丙泊酚溶液中计算得出的诱导药物剂量(PK组,n = 50);或1.5 μg/kg芬太尼用生理盐水稀释至2 mL(诱导前)加从11 mL丙泊酚溶液中计算得出的诱导药物剂量(PF组,n = 50)。两组中,均先静脉注射初始负荷剂量的丙泊酚1 mg/kg(为简化起见,假设注射器中仅含丙泊酚),随后进行调整输注以达到Ramsay镇静评分6分。平均动脉压(MAP)是主要结局指标。
PK组48例患者和PF组44例患者的数据可用于分析。PK组有7例患者(14.6%)出现低血压,而PF组有17例患者(38.6%)出现低血压(P = 0.009)。与基线相比,PF组术中MAP显著低于PK组。
在儿科急诊短时间外科手术中,就血流动力学稳定性和较低的呼吸暂停发生率而言,低剂量氯胺酮与丙泊酚联合使用比丙泊酚 - 芬太尼联合使用更有效且更安全。