Department of Surgery, University of California, San Francisco, CA, USA.
J Trauma Acute Care Surg. 2012 Jul;73(1):87-93. doi: 10.1097/TA.0b013e3182598c70.
Recent studies identify a survival benefit from the administration of antifibrinolytic agents in patients with severe injury and trauma. However, identification of hyperfibrinolysis requires thromboelastography, which is not widely available. We hypothesized that analysis of patients with thromboelastography-diagnosed hyperfibrinolysis would identify clinical criteria for empiric antifibrinolytic treatment in the absence of thromboelastography.
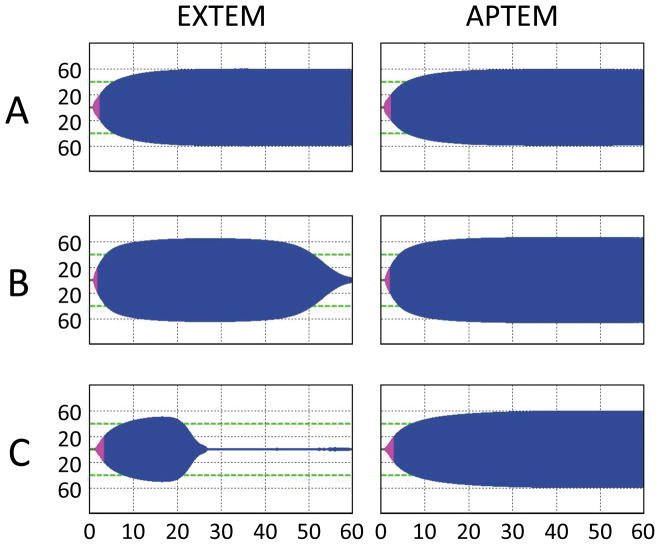
From November 2010 to March 2012, serial blood samples were collected from 115 patients with critical injury on arrival to the emergency department of an urban Level I trauma center. Rotational thromboelastography was performed to assess viscoelastic properties of clot formation in the presence and absence of aprotinin to identify treatable hyperfibrinolysis. For 20 patients identified with treatable hyperfibrinolysis, clinical predictors were investigated using receiver operating characteristic analysis.
Of the 115 patients evaluated, 20% had hyperfibrinolysis, defined as an admission maximal clot lysis of 10% or higher, reversible by aprotinin treatment. Patients with hyperfibrinolysis had significantly lower temperature, pH, and platelet counts and higher international normalized ratio, activated partial thromboplastin time, and D-dimer. Hyperfibrinolysis was associated with multiorgan failure (63.2% vs. 24.6%, p = 0.004) and mortality (52.2% vs. 12.9%, p < 0.001). We then evaluated all non-rotational thromboelastography clinical and laboratory parameters predictive of hyperfibrinolysis using receiver operating characteristic analysis to evaluate potential empiric treatment guidelines. The presence of hypothermia (temperature ≤36.0°C), acidosis (pH ≤7.2), relative coagulopathy (international normalized ratio ≥1.3 or activated partial thromboplastin time ≥30), or relative thrombocytopenia (platelet count ≤200) identified hyperfibrinolysis with 100% sensitivity and 55.4% specificity (area under the curve, 0.777).
Consideration of empiric antifibrinolytic therapy is warranted for patients with critical injury and trauma who present with acidosis, hypothermia, coagulopathy, or relative thrombocytopenia. These clinical predictors identified hyperfibrinolysis with 100% sensitivity while simultaneously eliminating 46.6% of inappropriate therapy compared with the empiric treatment of all injured patients. These criteria will facilitate empiric treatment of hyperfibrinolysis for clinicians without access to thromboelastography.
Prognostic study, level III.
最近的研究表明,在严重创伤和外伤患者中,使用抗纤维蛋白溶解剂治疗可提高生存率。然而,纤维蛋白溶解亢进的鉴定需要血栓弹性描记术,而这种技术并不广泛应用。我们假设,通过对血栓弹性描记术诊断为纤维蛋白溶解亢进的患者进行分析,可以确定在没有血栓弹性描记术的情况下经验性抗纤维蛋白溶解治疗的临床标准。
从 2010 年 11 月至 2012 年 3 月,对城市一级创伤中心急诊科收治的 115 名严重创伤患者连续采集血液样本。进行旋转血栓弹性描记术,以评估在存在和不存在抑肽酶的情况下血凝块形成的粘弹性特性,从而确定可治疗性纤维蛋白溶解亢进。对 20 例经抑肽酶治疗可逆转的可治疗性纤维蛋白溶解亢进患者进行临床预测因子分析。
在 115 例评估患者中,20%的患者出现纤维蛋白溶解亢进,表现为入院时最大纤维蛋白溶解率为 10%或更高,抑肽酶治疗后可逆转。纤维蛋白溶解亢进患者的体温、pH 值和血小板计数明显较低,而国际标准化比值、活化部分凝血活酶时间和 D-二聚体较高。纤维蛋白溶解亢进与多器官功能衰竭(63.2%比 24.6%,p=0.004)和死亡率(52.2%比 12.9%,p<0.001)相关。然后,我们使用受试者工作特征分析评估所有非旋转血栓弹性描记术的临床和实验室参数,以预测纤维蛋白溶解亢进的可能性,评估潜在的经验性治疗指南。存在低体温(体温≤36.0°C)、酸中毒(pH≤7.2)、相对凝血障碍(国际标准化比值≥1.3 或活化部分凝血活酶时间≥30)或相对血小板减少症(血小板计数≤200)时,可 100%敏感、55.4%特异度(曲线下面积 0.777)识别纤维蛋白溶解亢进。
对于出现酸中毒、低体温、凝血障碍或相对血小板减少症的严重创伤和外伤患者,应考虑经验性抗纤维蛋白溶解治疗。这些临床预测因子可 100%敏感地识别纤维蛋白溶解亢进,同时与对所有受伤患者进行经验性治疗相比,可同时消除 46.6%的不适当治疗。这些标准将有助于在没有血栓弹性描记术的情况下为临床医生提供经验性纤维蛋白溶解亢进治疗。
预后研究,III 级。