Immpact, University of Aberdeen, Aberdeen, Scotland.
PLoS Med. 2012;9(7):e1001264. doi: 10.1371/journal.pmed.1001264. Epub 2012 Jul 10.
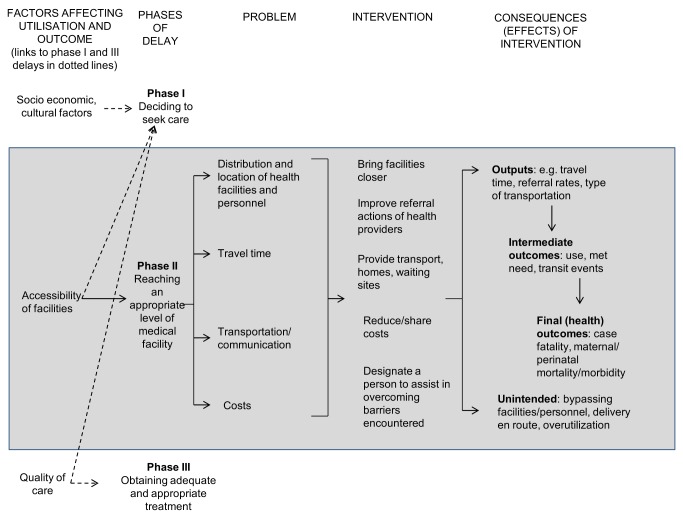
Pregnancy complications can be unpredictable and many women in developing countries cannot access health facilities where life-saving care is available. This study assesses the effects of referral interventions that enable pregnant women to reach health facilities during an emergency, after the decision to seek care is made.
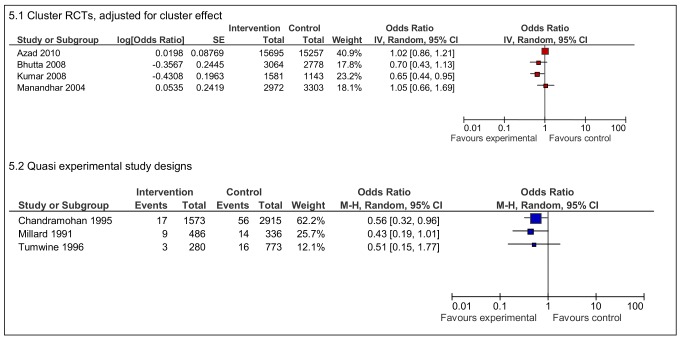
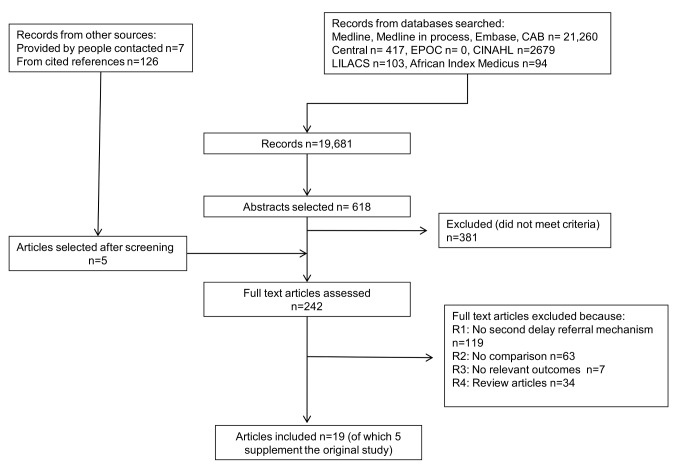
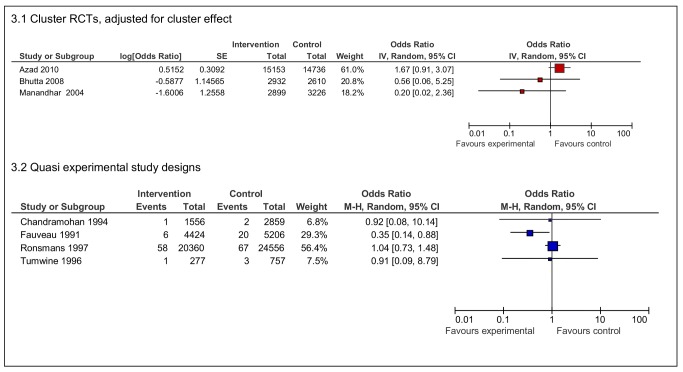
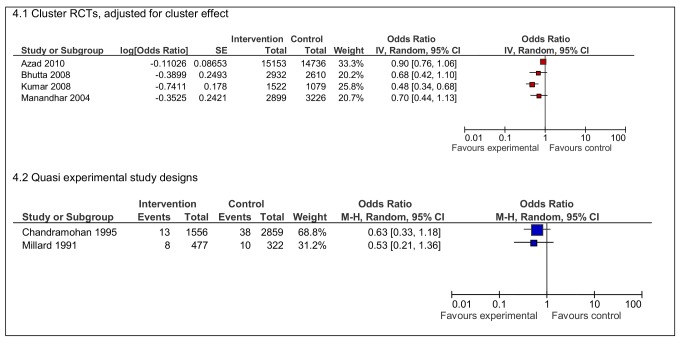
Selected bibliographic databases were searched with no date or language restrictions. Randomised controlled trials and quasi experimental study designs with a comparison group were included. Outcomes of interest included maternal and neonatal mortality and other intermediate measures such as service utilisation. Two reviewers independently selected, appraised, and extracted articles using predefined fields. Forest plots, tables, and qualitative summaries of study quality, size, and direction of effect were used for analysis. Nineteen studies were included. In South Asian settings, four studies of organisational interventions in communities that generated funds for transport reduced neonatal deaths, with the largest effect seen in India (odds ratio 0·48 95% CI 0·34-0·68). Three quasi experimental studies from sub-Saharan Africa reported reductions in stillbirths with maternity waiting home interventions, with one statistically significant result (OR 0.56 95% CI 0.32-0.96). Effects of interventions on maternal mortality were unclear. Referral interventions usually improved utilisation of health services but the opposite effect was also documented. The effects of multiple interventions in the studies could not be disentangled. Explanatory mechanisms through which the interventions worked could not be ascertained.
Community mobilisation interventions may reduce neonatal mortality but the contribution of referral components cannot be ascertained. The reduction in stillbirth rates resulting from maternity waiting homes needs further study. Referral interventions can have unexpected adverse effects. To inform the implementation of effective referral interventions, improved monitoring and evaluation practices are necessary, along with studies that develop better understanding of how interventions work.
妊娠并发症可能难以预测,许多发展中国家的妇女无法获得可提供救生护理的卫生机构。本研究评估了使孕妇在决定寻求护理后能够在紧急情况下到达卫生机构的转介干预措施的效果。
对选定的文献数据库进行了无日期和语言限制的检索。纳入了随机对照试验和具有对照组的准实验研究设计。感兴趣的结果包括孕产妇和新生儿死亡率以及服务利用等其他中间指标。两名审查员独立使用预定义字段选择、评估和提取文章。使用森林图、表格和研究质量、大小和效应方向的定性总结进行分析。纳入了 19 项研究。在南亚地区,四项针对社区的组织干预措施研究为交通提供资金,降低了新生儿死亡,其中印度的效果最大(比值比 0.48,95%置信区间 0.34-0.68)。三项来自撒哈拉以南非洲的准实验研究报告了产妇等候之家干预措施可降低死产,其中一项具有统计学意义(比值比 0.56,95%置信区间 0.32-0.96)。干预措施对孕产妇死亡率的影响尚不清楚。转介干预措施通常会增加卫生服务的利用,但也有相反的结果。研究中多种干预措施的效果无法区分。无法确定干预措施发挥作用的解释机制。
社区动员干预措施可能会降低新生儿死亡率,但无法确定转介部分的贡献。产妇等候之家导致的死产率降低需要进一步研究。转介干预措施可能会产生意想不到的不利影响。为了为实施有效的转介干预措施提供信息,需要改进监测和评估实践,并开展研究以更好地了解干预措施的工作原理。