Department of Public and Occupational Health, VU University Medical Centre, Amsterdam, The Netherlands.
BMC Palliat Care. 2012 Aug 1;11:12. doi: 10.1186/1472-684X-11-12.
Unbearable suffering most frequently is reported in end-of-life cancer patients in primary care. However, research seldom addresses unbearable suffering. The aim of this study was to comprehensively investigate the various aspects of unbearable suffering in end-of-life cancer patients cared for in primary care.
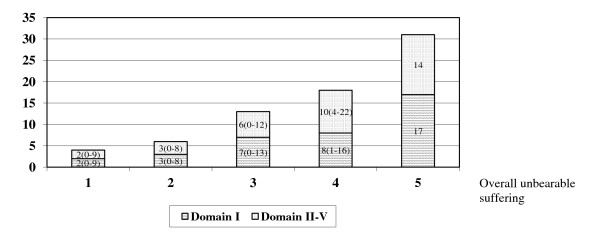
Forty four general practitioners recruited end-of-life cancer patients with an estimated life expectancy of half a year or shorter. The inclusion period was three years, follow-up lasted one additional year. Practices were monitored bimonthly to identify new cases. Unbearable aspects in five domains and overall unbearable suffering were quantitatively assessed (5-point scale) through patient interviews every two months with a comprehensive instrument. Scores of 4 (serious) or 5 (hardly can be worse) were defined unbearable. The last interviews before death were analyzed. Sources providing strength to bear suffering were identified through additional open-ended questions.
Seventy six out of 148 patients (51%) requested to participate consented; the attrition rate was 8%, while 8% were alive at the end of follow-up. Sixty four patients were followed up until death; in 60 patients interviews were complete. Overall unbearable suffering occurred in 28%. A mean of 18 unbearable aspects was present in patients with serious (score 4) overall unbearable suffering. Overall, half of the unbearable aspects involved the domain of traditional medical symptoms. The most frequent unbearable aspects were weakness, general discomfort, tiredness, pain, loss of appetite and not sleeping well (25%-57%). The other half of the unbearable aspects involved the domains of function, personhood, environment, and nature and prognosis of disease. The most frequent unbearable aspects were impaired activities, feeling dependent, help needed with housekeeping, not being able to do important things, trouble accepting the situation, being bedridden and loss of control (27%-55%). The combination of love and support was the most frequent source (67%) providing strength to bear suffering.
Overall unbearable suffering occurred in one in every four end-of-life cancer patients. Half of the unbearable aspects involved medical symptoms, the other half concerned psychological, social and existential dimensions. Physicians need to comprehensively assess suffering and provide psychosocial interventions alongside physical symptom management.
在初级保健机构中临终的癌症患者经常报告无法忍受的痛苦。然而,研究很少涉及无法忍受的痛苦。本研究的目的是全面调查初级保健中临终的癌症患者的各个方面的无法忍受的痛苦。
44 名全科医生招募了预计生存期为半年或更短的临终癌症患者。纳入期为 3 年,随访期为 1 年。每两个月对实践进行监测,以确定新病例。通过患者访谈,使用综合工具,每两个月对五个领域的无法忍受的方面和整体无法忍受的痛苦进行定量评估(5 分制)。得分 4(严重)或 5(几乎无法更糟)定义为无法忍受。在死亡前的最后一次访谈中进行了分析。通过附加的开放式问题确定提供承受痛苦的力量的来源。
在 148 名患者中,有 76 名(51%)要求参加并同意;失访率为 8%,而在随访结束时,8%的患者仍存活。64 名患者接受了随访直到死亡;在 60 名患者中,访谈是完整的。整体无法忍受的痛苦发生率为 28%。在有严重(评分 4)整体无法忍受的痛苦的患者中,存在平均 18 个无法忍受的方面。总体而言,一半的无法忍受的方面涉及传统医疗症状领域。最常见的无法忍受的方面是虚弱、全身不适、疲倦、疼痛、食欲不振和睡眠不佳(25%-57%)。另一半无法忍受的方面涉及功能、人格、环境以及疾病的性质和预后。最常见的无法忍受的方面是活动受限、依赖感、需要帮助做家务、无法做重要的事情、难以接受情况、卧床不起和失去控制(27%-55%)。爱和支持的结合是提供承受痛苦力量的最常见来源(67%)。
每四个临终的癌症患者中就有一个出现整体无法忍受的痛苦。一半的无法忍受的方面涉及医疗症状,另一半则涉及心理、社会和存在维度。医生需要全面评估痛苦,并提供心理社会干预,同时进行身体症状管理。