NIHR Oxford Biomedical Research Centre, John Radcliffe Hospital, Oxford, United Kingdom.
PLoS Med. 2012;9(7):e1001279. doi: 10.1371/journal.pmed.1001279. Epub 2012 Jul 31.
Changing clinical impact, as virulent clones replace less virulent ones, is a feature of many pathogenic bacterial species and can be difficult to detect. Consequently, innovative techniques monitoring infection severity are of potential clinical value.
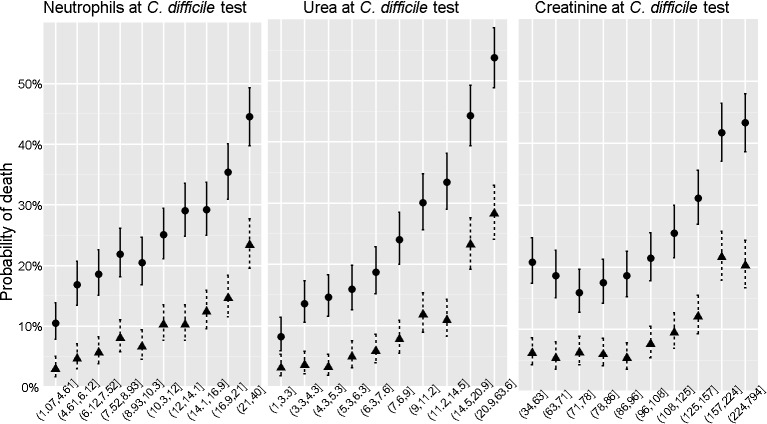
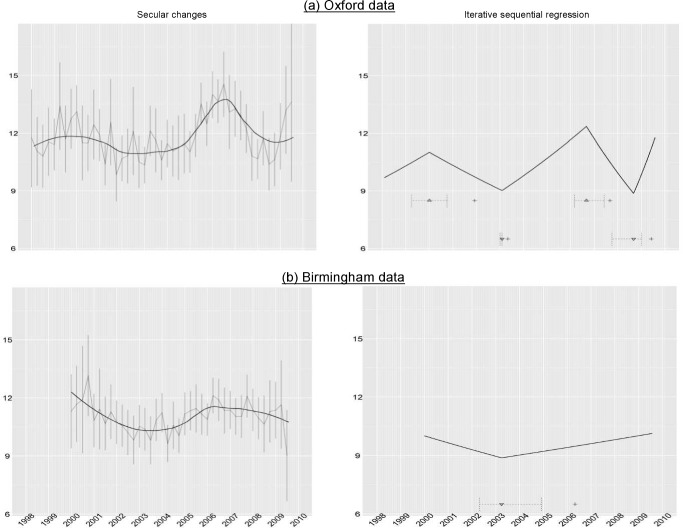
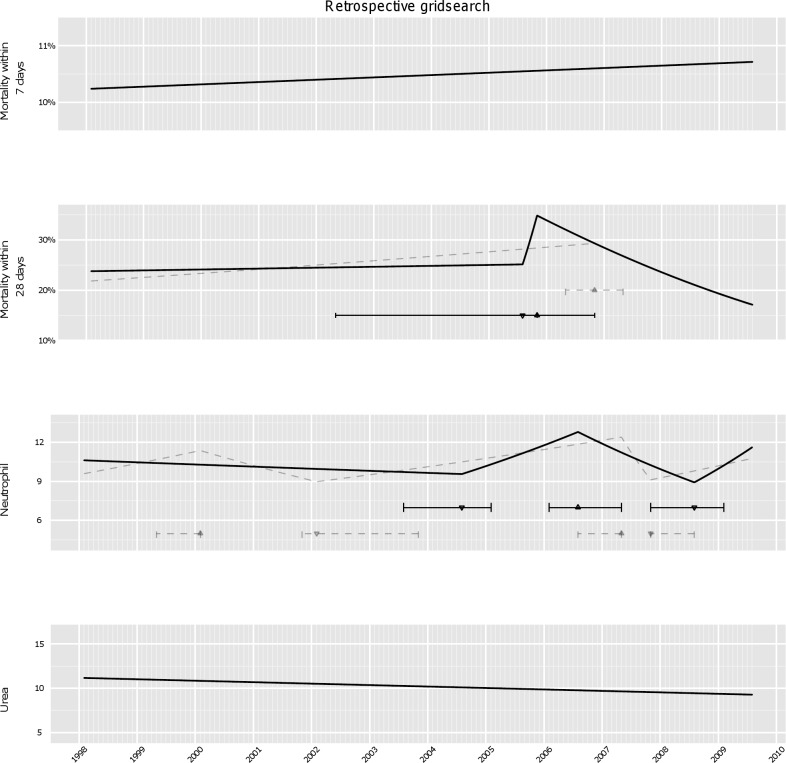
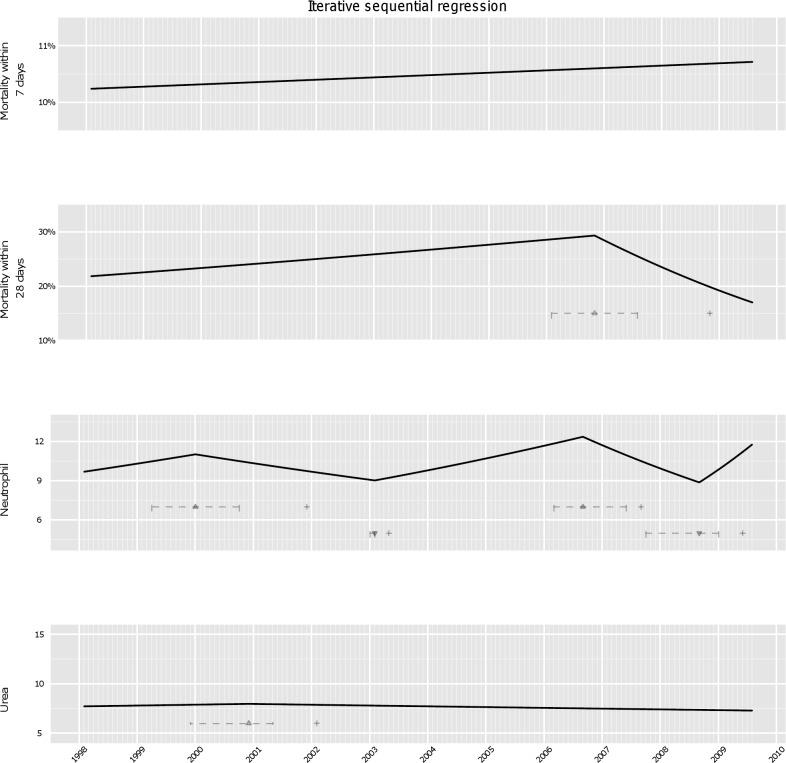
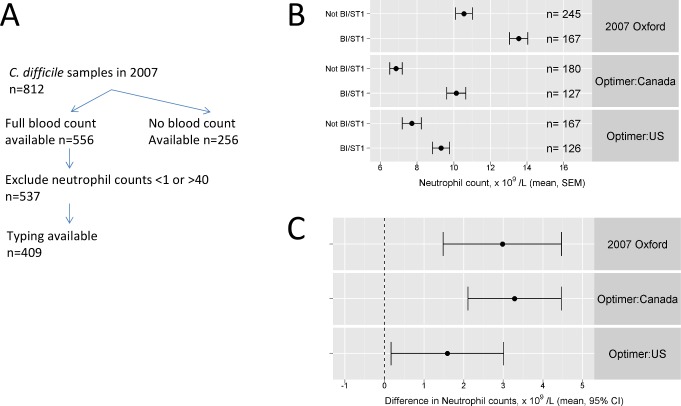
We studied 5,551 toxin-positive and 20,098 persistently toxin-negative patients tested for Clostridium difficile infection between February 1998 and July 2009 in a group of hospitals based in Oxford, UK, and investigated 28-day mortality and biomarkers of inflammation (blood neutrophil count, urea, and creatinine concentrations) collected at diagnosis using iterative sequential regression (ISR), a novel joinpoint-based regression technique suitable for serial monitoring of continuous or dichotomous outcomes. Among C. difficile toxin-positive patients in the Oxford hospitals, mean neutrophil counts on diagnosis increased from 2003, peaked in 2006-2007, and then declined; 28-day mortality increased from early 2006, peaked in late 2006-2007, and then declined. Molecular typing confirmed these changes were likely due to the ingress of the globally distributed severe C. difficile strain, ST1. We assessed the generalizability of ISR-based severity monitoring in three ways. First, we assessed and found strong (p<0.0001) associations between isolation of the ST1 severe strain and higher neutrophil counts at diagnosis in two unrelated large multi-centre studies, suggesting the technique described might be useful elsewhere. Second, we assessed and found similar trends in a second group of hospitals in Birmingham, UK, from which 5,399 cases were analysed. Third, we used simulation to assess the performance of this surveillance system given the ingress of future severe strains under a variety of assumptions. ISR-based severity monitoring allowed the detection of the severity change years earlier than mortality monitoring.
Automated electronic systems providing early warning of the changing severity of infectious conditions can be established using routinely collected laboratory hospital data. In the settings studied here these systems have higher performance than those monitoring mortality, at least in C. difficile infection. Such systems could have wider applicability for monitoring infections presenting in hospital.
随着毒力更强的克隆体取代毒力较弱的克隆体,临床影响发生变化是许多病原细菌的特征,而且这种变化很难被检测到。因此,监测感染严重程度的创新技术具有潜在的临床价值。
我们研究了在英国牛津的一组医院中,1998 年 2 月至 2009 年 7 月间接受检测的 5551 例产毒素阳性和 20098 例持续产毒素阴性的艰难梭菌感染患者,使用迭代序列回归(ISR),一种适合连续或二分连续结果的新型基于连接点的回归技术,研究了诊断时的 28 天死亡率和炎症生物标志物(血液中性粒细胞计数、尿素和肌酐浓度)。在牛津医院的产毒素阳性艰难梭菌感染患者中,诊断时的中性粒细胞计数从 2003 年开始增加,在 2006-2007 年达到峰值,然后下降;28 天死亡率从 2006 年初开始上升,在 2006-2007 年末达到峰值,然后下降。分子分型证实这些变化可能是由于全球分布的严重艰难梭菌菌株 ST1 的传入。我们通过三种方式评估了基于 ISR 的严重程度监测的普遍性。首先,我们评估并发现,在两项独立的大型多中心研究中,ST1 严重菌株的分离与诊断时更高的中性粒细胞计数之间存在强烈的(p<0.0001)关联,这表明所描述的技术可能在其他地方有用。其次,我们评估并发现,在英国伯明翰的第二组医院中也存在类似的趋势,对其中的 5399 例病例进行了分析。第三,我们使用模拟来评估在各种假设下未来严重菌株传入时这种监测系统的性能。基于 ISR 的严重程度监测比死亡率监测更早地检测到感染严重程度的变化。
使用常规收集的实验室医院数据,可以建立自动电子系统,为不断变化的传染病严重程度提供早期预警。在研究的环境中,这些系统在监测艰难梭菌感染方面的性能优于监测死亡率的系统。此类系统可更广泛地应用于监测住院感染。