Umeå Centre for Global Health Research, Umeå University, Umeå, Sweden.
Glob Health Action. 2012;5. doi: 10.3402/gha.v5i0.17989. Epub 2012 Aug 3.
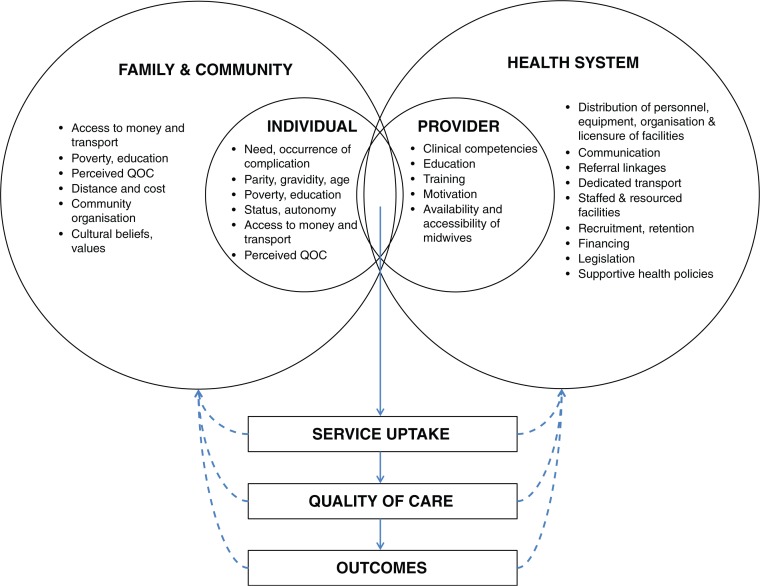
Estimates suggest that over 350,000 deaths and more than 20 million severe disabilities result from the complications of pregnancy, childbirth or its management each year. Death and disability occur predominately among disadvantaged women in resource-poor settings and are largely preventable with adequate delivery care. This paper presents the substantive findings and policy implications from a programme of PhD research, of which the overarching objective was to assess quality of, and access to, care in obstetric emergencies. Three critical incident audits were conducted in two rural districts on Java, Indonesia: a confidential enquiry, a verbal autopsy survey, and a community-based review. The studies examined cases of maternal mortality and severe morbidity from the perspectives of local service users and health providers. A range of inter-related determining factors was identified. When unexpected delivery complications occurred, women and families were often uninformed, unprepared, found care unavailable, unaffordable, and many relied on traditional providers. Midwives in villages made important contributions by stabilising women and facilitating referrals but were often scarce in remote areas and lacked sufficient clinical competencies and payment incentives to treat the poor. Emergency transport was often unavailable and private transport was unreliable and incurred costs. In facilities, there was a reluctance to admit poorer women and those accepted were often admitted to ill-equipped, under-staffed wards. As a result, referrals between hospitals were also common. Otherwise, social health insurance, designed to reduce financial barriers, was particularly problematic, constraining quality and access within and outside facilities. Health workers and service users provided rich and explicit assessments of care and outcomes. These were used to develop a conceptual model in which quality and access are conceived of as social processes, observable through experience and reflective of the broader relationships between individuals and health systems. According to this model, differential quality and access can become both socially legitimate (imposed by structural arrangements) and socially legitimised (reciprocally maintained through the actions of individuals). This interpretation suggests that in a context of commodified care provision, adverse obstetric outcomes will occur and recur for disadvantaged women. Health system reform should focus on the unintended effects of market-based service provision to exclude those without the ability to pay for delivery care directly.
据估计,每年有超过 35 万人死于妊娠、分娩或其管理的并发症,2000 多万人因此严重残疾。死亡和残疾主要发生在资源匮乏环境中处于不利地位的妇女中,通过适当的分娩护理,这些情况大多可以预防。本文介绍了博士研究计划的实质性研究结果和政策影响,该计划的总体目标是评估产科急症护理的质量和可及性。在印度尼西亚爪哇的两个农村地区进行了三次关键事件审核:机密调查、口头尸检调查和基于社区的审查。这些研究从当地服务使用者和卫生提供者的角度检查了孕产妇死亡和严重发病的病例。确定了一系列相互关联的决定因素。当出现意外分娩并发症时,妇女和家庭往往得不到通知,没有准备,找不到护理服务,负担不起费用,许多人依赖传统的提供者。村里的助产士通过稳定妇女和促进转诊做出了重要贡献,但在偏远地区往往稀缺,缺乏足够的临床能力和支付激励来治疗穷人。紧急交通往往不可用,私人交通不可靠且费用高昂。在医疗机构中,不愿意收治较贫困的妇女,而那些被收治的妇女往往被收治在设备简陋、人手不足的病房。因此,医院之间的转诊也很常见。否则,旨在减少经济障碍的社会健康保险,特别是有问题的,限制了设施内外的质量和可及性。卫生工作者和服务使用者对护理和结果进行了丰富而明确的评估。这些评估被用于开发一个概念模型,其中质量和可及性被视为社会过程,可以通过经验观察到,并反映个人与卫生系统之间的更广泛关系。根据该模型,不同的质量和可及性可能会变得既具有社会合法性(由结构安排强加),又具有社会合法性(通过个人的行动相互维持)。这种解释表明,在以市场为基础的护理提供商品化的背景下,弱势妇女的不良产科结局将继续发生。卫生系统改革应侧重于市场导向的服务提供的意外影响,以排除那些没有直接支付分娩护理费用能力的人。