Emergency Department Azienda Ospedaliera Sant'Andrea, School of Medicine and Psychology Sapienza Univesity, Rome, Italy.
BMC Infect Dis. 2012 Aug 8;12:184. doi: 10.1186/1471-2334-12-184.
The aim of our study was to evaluate the prognostic value of MR-proADM and PCT levels in febrile patients in the ED in comparison with a disease severity index score, the APACHE II score. We also evaluated the ability of MR-proADM and PCT to predict hospitalization.
This was an observational, multicentric study. We enrolled 128 patients referred to the ED with high fever and a suspicion of severe infection such as sepsis, lower respiratory tract infections, urinary tract infections, gastrointestinal infections, soft tissue infections, central nervous system infections, or osteomyelitis. The APACHE II score was calculated for each patient.
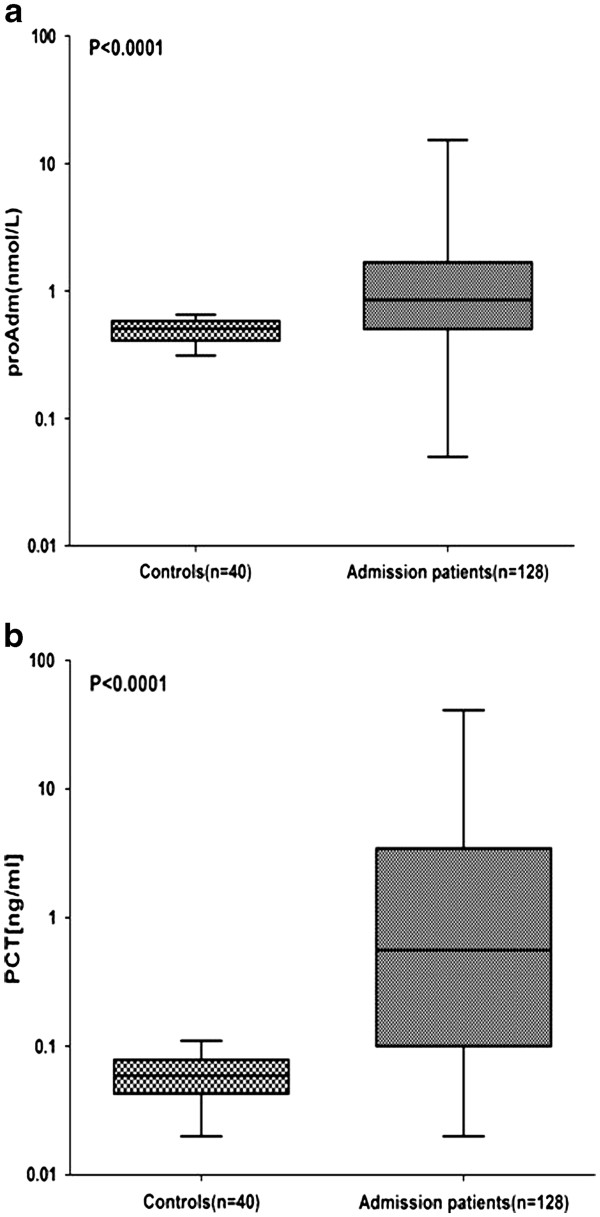
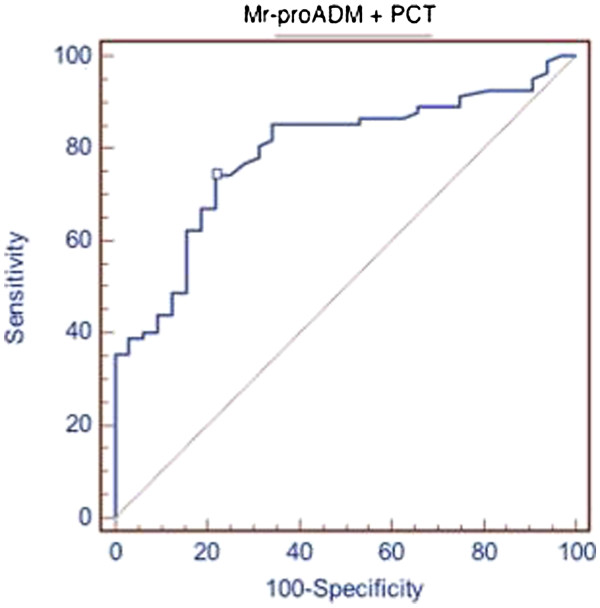
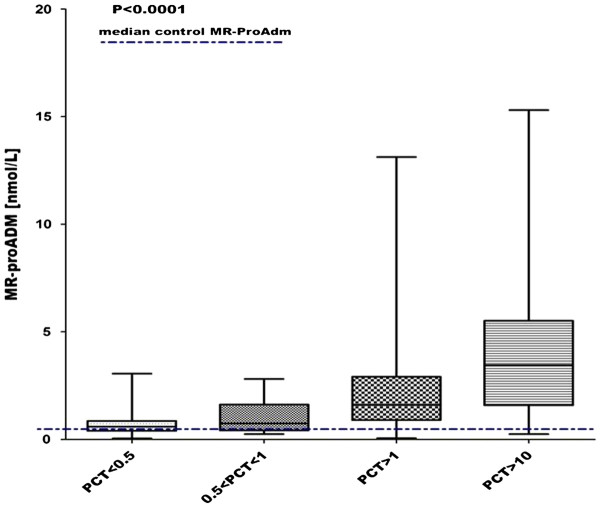
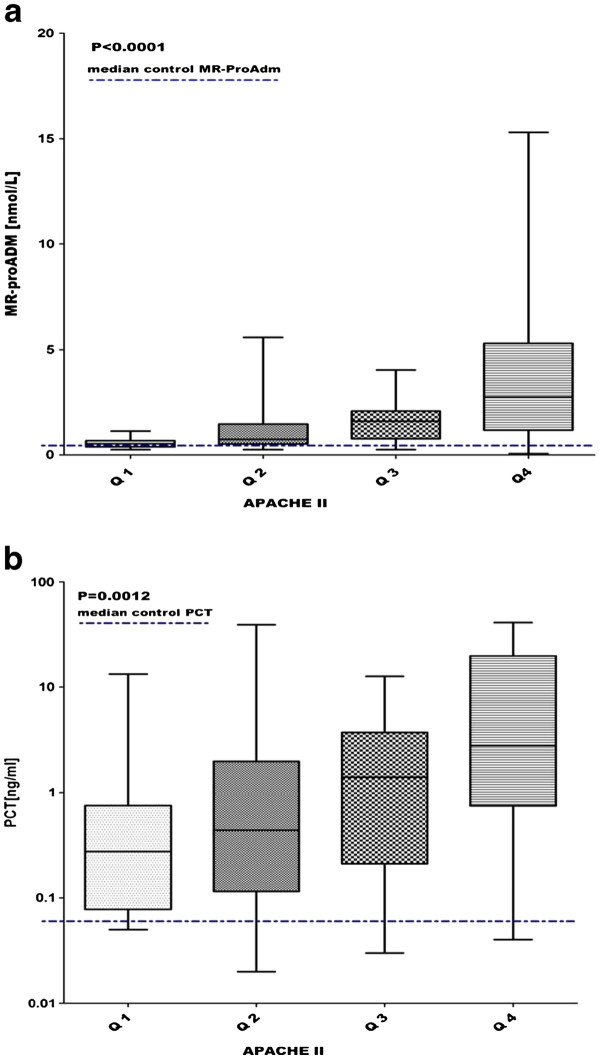
MR-proADM median values in controls were 0.5 nmol/l as compared with 0.85 nmol/l in patients (P < 0.0001), while PCT values in controls were 0.06 ng/ml versus 0.56 ng/ml in patients (P < 0.0001). In all patients there was a statistically significant stepwise increase in MR-proADM levels in accordance with PCT values (P < 0.0001). MR-proADM and PCT levels were significantly increased in accordance with the Apache II quartiles (P < 0.0001 and P = 0.0012 respectively).In the respiratory infections, urinary infections, and sepsis-septic shock groups we found a correlation between the Apache II and MR-proADM respectively and MR-proADM and PCT respectively. We evaluated the ability of MR-proADM and PCT to predict hospitalization in patients admitted to our emergency departments complaining of fever. MR-proADM alone had an AUC of 0.694, while PCT alone had an AUC of 0.763. The combined use of PCT and MR-proADM instead showed an AUC of 0.79.
The present study highlights the way in which MR-proADM and PCT may be helpful to the febrile patient's care in the ED. Our data support the prognostic role of MR-proADM and PCT in that setting, as demonstrated by the correlation with the APACHE II score. The combined use of the two biomarkers can predict a subsequent hospitalization of febrile patients. The rational use of these two molecules could lead to several advantages, such as faster diagnosis, more accurate risk stratification, and optimization of the treatment, with consequent benefit to the patient and considerably reduced costs.
我们的研究目的是评估 MR-proADM 和 PCT 水平在急诊发热患者中的预后价值,并与疾病严重程度指数评分(APACHE II 评分)进行比较。我们还评估了 MR-proADM 和 PCT 预测住院的能力。
这是一项观察性、多中心研究。我们招募了 128 名因高热和疑似严重感染(如败血症、下呼吸道感染、尿路感染、胃肠道感染、软组织感染、中枢神经系统感染或骨髓炎)而被转至急诊的患者。为每位患者计算 APACHE II 评分。
对照组的 MR-proADM 中位数为 0.5 nmol/L,而患者组为 0.85 nmol/L(P<0.0001),对照组的 PCT 值为 0.06 ng/ml,而患者组为 0.56 ng/ml(P<0.0001)。在所有患者中,MR-proADM 水平与 PCT 值呈显著逐步升高(P<0.0001)。MR-proADM 和 PCT 水平与 Apache II 四分位数呈显著升高(P<0.0001 和 P=0.0012)。在呼吸道感染、尿路感染和败血症-感染性休克组中,我们发现 Apache II 与 MR-proADM 之间以及 MR-proADM 与 PCT 之间存在相关性。我们评估了在因发热而被收入我院急诊的患者中,MR-proADM 和 PCT 预测住院的能力。MR-proADM 单独的 AUC 为 0.694,而 PCT 单独的 AUC 为 0.763。PCT 和 MR-proADM 联合使用的 AUC 为 0.79。
本研究强调了 MR-proADM 和 PCT 可能有助于急诊发热患者的治疗。我们的数据支持 MR-proADM 和 PCT 在该环境中的预后作用,这表现在它们与 APACHE II 评分的相关性上。这两种生物标志物的联合使用可以预测发热患者随后的住院情况。这两种分子的合理使用可以带来许多优势,例如更快的诊断、更准确的风险分层和治疗优化,从而使患者受益,并显著降低成本。