Childhood Cancer Research Group, Department of Paediatrics, University of Oxford, Oxford OX3 7LG, UK.
Br J Cancer. 2012 Sep 25;107(7):1159-62. doi: 10.1038/bjc.2012.296. Epub 2012 Aug 16.
Increases in recorded childhood cancer incidence are widely reported, but do not necessarily represent real increases in risk. Time trends might conceal underlying steps caused by changes in diagnosis and registration procedures.
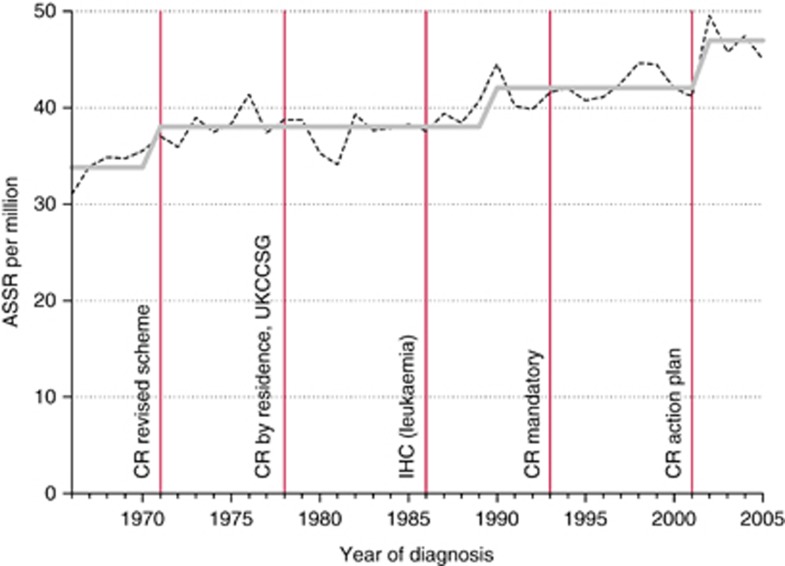
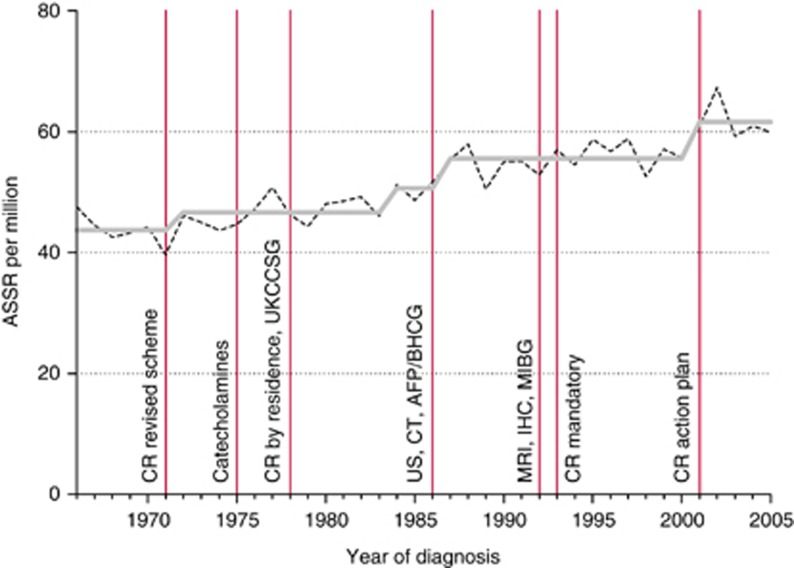
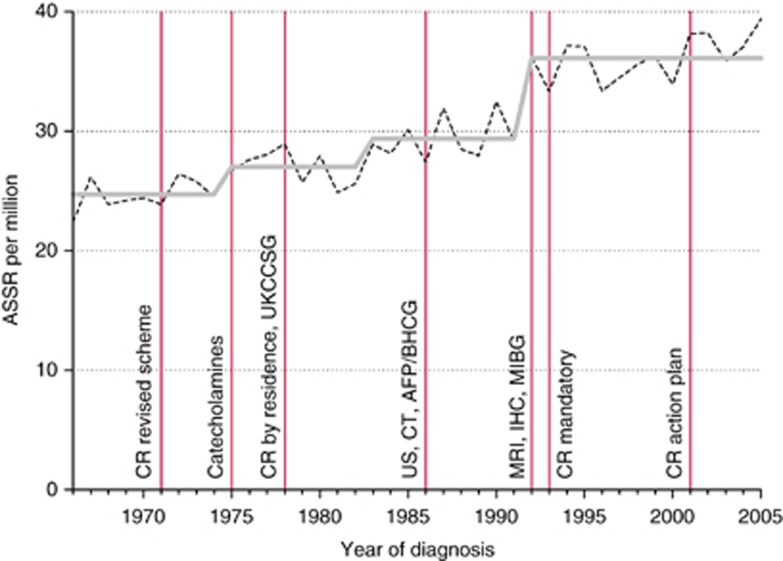
Using records from the National Registry of Childhood Tumours 1966-2005 (N=54650), the age-sex-standardised rate for residents of Great Britain aged under 15 years was calculated by individual year of diagnosis for each cancer subtype, and the average annual percentage change (trend) was assessed. The timing of assumed step changes in rate was estimated by iterative Poisson regression, and compared graphically with the approximate timing of innovations previously identified from published sources.
Estimated timing of underlying steps approximately coincided with the following relevant innovations: biochemical assays, mid-1980s (hepatic and germ-cell cancer); diagnostic imaging, mid-1980s to early 1990s (intracranial/intraspinal tumours, neuroblastoma, soft-tissue sarcoma); revised cancer registration scheme, 1971 (leukaemia, bone and soft-tissue sarcoma); mandatory registration, 1993 (intracranial/intraspinal tumours, retinoblastoma, melanoma/carcinoma); cancer registration improvements, 2001 (leukaemia, renal and hepatic cancer).
While the possibility of some real change in risk cannot be excluded, for many cancer subtypes the estimated timing of underlying step changes in rate appeared to correspond with changes in diagnosis or registration procedures. Childhood cancer may have been considerably under-recorded in the past.
有广泛报道称儿童癌症发病率的上升,但这并不一定代表风险的真实增加。时间趋势可能掩盖了由于诊断和登记程序变化而导致的潜在变化。
使用 1966-2005 年国家儿童肿瘤登记处(N=54650)的记录,计算了居住在英国的 15 岁以下人群的每一种癌症亚型的年龄性别标准化率,并评估了平均年百分比变化(趋势)。通过迭代泊松回归估计了假设的发病率变化的时间点,并与以前从已发表的资料中确定的创新的近似时间进行了图形比较。
潜在变化的估计时间点与以下相关创新基本一致:生化检测,20 世纪 80 年代中期(肝和生殖细胞瘤);诊断成像,20 世纪 80 年代中期至 90 年代初(颅内/脊髓肿瘤、神经母细胞瘤、软组织肉瘤);修订的癌症登记方案,1971 年(白血病、骨和软组织肉瘤);强制性登记,1993 年(颅内/脊髓肿瘤、视网膜母细胞瘤、黑素瘤/癌);癌症登记改进,2001 年(白血病、肾和肝肿瘤)。
虽然不能排除风险的某些真实变化的可能性,但对于许多癌症亚型,发病率潜在变化的估计时间似乎与诊断或登记程序的变化相对应。过去儿童癌症的记录可能有很大的遗漏。