Centre for Cancer Prevention, Wolfson Institute of Preventive Medicine, Queen Mary University of London, London EC1M 6BQ, UK.
BMJ. 2012 Aug 16;345:e5174. doi: 10.1136/bmj.e5174.
To explore the association between preterm delivery and treatment at colposcopy.
Retrospective-prospective cohort study using record linkage.
12 National Health Service hospitals in England.
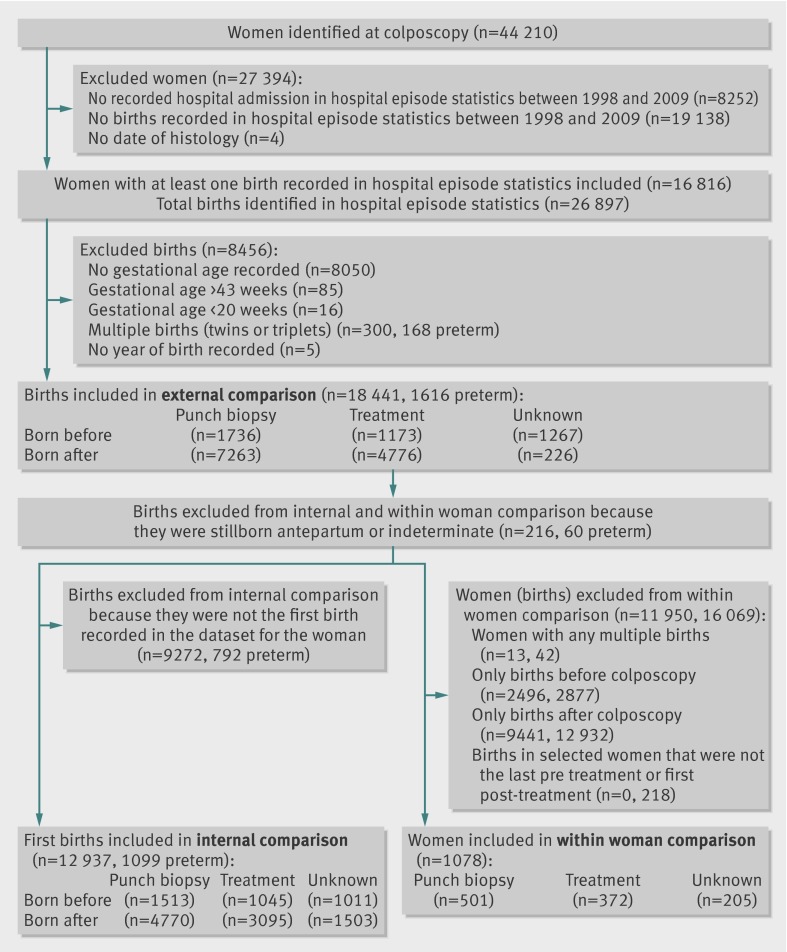
Women who had a cervical histology sample taken between 1987 and 2009. These women were linked by hospital episode statistics to hospital obstetric records between 1998 and 2009 for the whole of England to identify singleton live births between 20-43 gestational weeks before or after cervical histology.
Proportion of preterm births (<37 weeks); the relative risk for the strength of association between preterm births and treatment for cervical intraepithelial neoplasia.
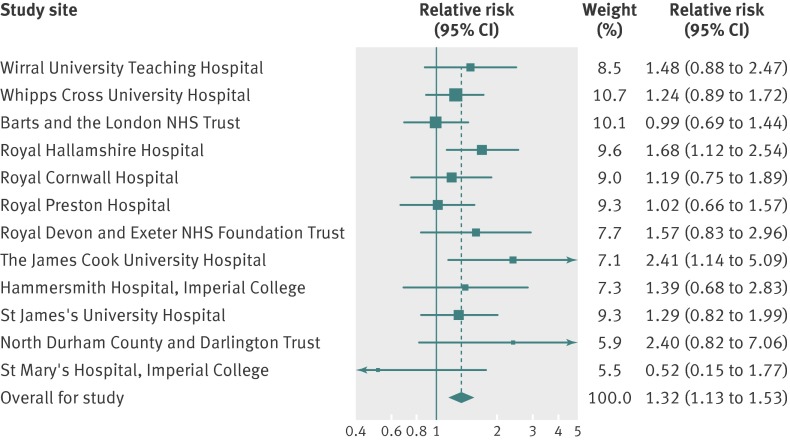
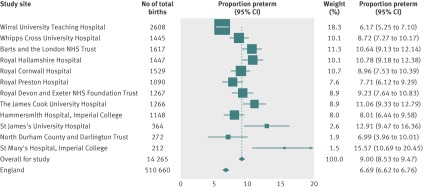
18,441 singleton births occurred: 4176 before histology and 14,265 after histology. Of the singleton births after histology, 9.0% (n=1284) were preterm compared with 6.7% of all births in England over the same period (excess risk 2.3 per 100 births, 95% confidence interval 1.8% to 2.8%). Among first births after histology, the adjusted relative risk associated with previous treatment was 1.19 (95% confidence interval 1.01 to 1.41); among first births before histology the relative risk associated with subsequent treatment was 1.47 (1.05 to 2.05). Combining these, the relative risk associated with treatment adjusted for timing relative to histology was 0.91 (0.66 to 1.26) corresponding to an absolute difference of -0.25 (-2.61 to 2.11) per 100 singleton births. Among 372 women who gave birth both before and after treatment, there were 30 preterm births after treatment and 32 before treatment (relative risk 0.94, 0.62 to 1.43).
The risk of preterm delivery in women treated by colposcopy in England was substantially less than that in many other studies, predominantly from Nordic countries. The increased risk may be a consequence of confounding and not caused by treatment. Although this study is reassuring for large loop excision of the transformation zone overall, it is possible that deep conisation or repeated treatment leads to an increased risk of preterm delivery.
探讨早产与阴道镜检查治疗的关系。
采用病历链接的回顾性前瞻性队列研究。
英格兰 12 家国民保健服务医院。
1987 年至 2009 年间进行宫颈组织学样本检测的女性。通过医院入院统计数据,将这些女性与 1998 年至 2009 年英格兰所有医院的产科记录相关联,以确定在宫颈组织学检查前或后 20-43 孕周内的单胎活产。
早产率(<37 周);早产与宫颈上皮内瘤变治疗之间关联强度的相对风险。
18441 例单胎分娩发生:组织学检查前 4176 例,组织学检查后 14265 例。在组织学检查后的单胎分娩中,9.0%(n=1284)为早产,而同期英格兰所有分娩中这一比例为 6.7%(每 100 例分娩中早产风险增加 2.3,95%置信区间 1.8%至 2.8%)。在组织学检查后的首次分娩中,既往治疗的校正后相对风险为 1.19(95%置信区间 1.01 至 1.41);而在组织学检查前的首次分娩中,随后治疗的相对风险为 1.47(1.05 至 2.05)。将两者结合起来,相对于组织学检查的治疗调整后相对风险为 0.91(0.66 至 1.26),相当于每 100 例单胎分娩的绝对差异为-0.25(-2.61 至 2.11)。在 372 例接受治疗前后分娩的女性中,治疗后有 30 例早产,治疗前有 32 例(相对风险 0.94,0.62 至 1.43)。
在英格兰接受阴道镜检查治疗的女性中,早产风险明显低于许多其他研究,这些研究主要来自北欧国家。增加的风险可能是混杂因素的结果,而不是治疗引起的。尽管这项研究总体上对环形电切术治疗转化区有较大的保证,但深度锥切或反复治疗可能导致早产风险增加。