Knowledge Translation Unit, University of Cape Town Lung Institute, University of Cape Town, Cape Town, South Africa.
Lancet. 2012 Sep 8;380(9845):889-98. doi: 10.1016/S0140-6736(12)60730-2. Epub 2012 Aug 15.
Robust evidence of the effectiveness of task shifting of antiretroviral therapy (ART) from doctors to other health workers is scarce. We aimed to assess the effects on mortality, viral suppression, and other health outcomes and quality indicators of the Streamlining Tasks and Roles to Expand Treatment and Care for HIV (STRETCH) programme, which provides educational outreach training of nurses to initiate and represcribe ART, and to decentralise care.
We undertook a pragmatic, parallel, cluster-randomised trial in South Africa between Jan 28, 2008, and June 30, 2010. We randomly assigned 31 primary-care ART clinics to implement the STRETCH programme (intervention group) or to continue with standard care (control group). The ratio of randomisation depended on how many clinics were in each of nine strata. Two cohorts were enrolled: eligible patients in cohort 1 were adults (aged ≥16 years) with CD4 counts of 350 cells per μL or less who were not receiving ART; those in cohort 2 were adults who had already received ART for at least 6 months and were being treated at enrolment. The primary outcome in cohort 1 was time to death (superiority analysis). The primary outcome in cohort 2 was the proportion with undetectable viral loads (<400 copies per mL) 12 months after enrolment (equivalence analysis, prespecified difference <6%). Patients and clinicians could not be masked to group assignment. The interim analysis was blind, but data analysts were not masked after the database was locked for final analysis. Analyses were done by intention to treat. This trial is registered, number ISRCTN46836853.
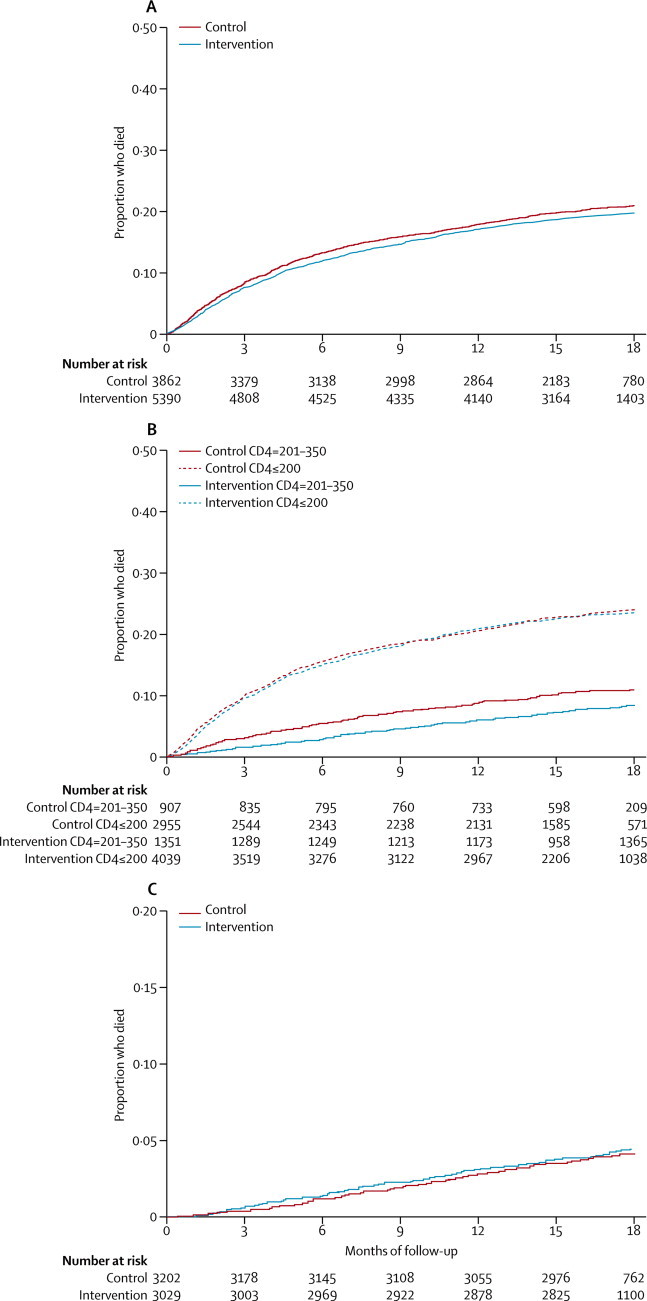
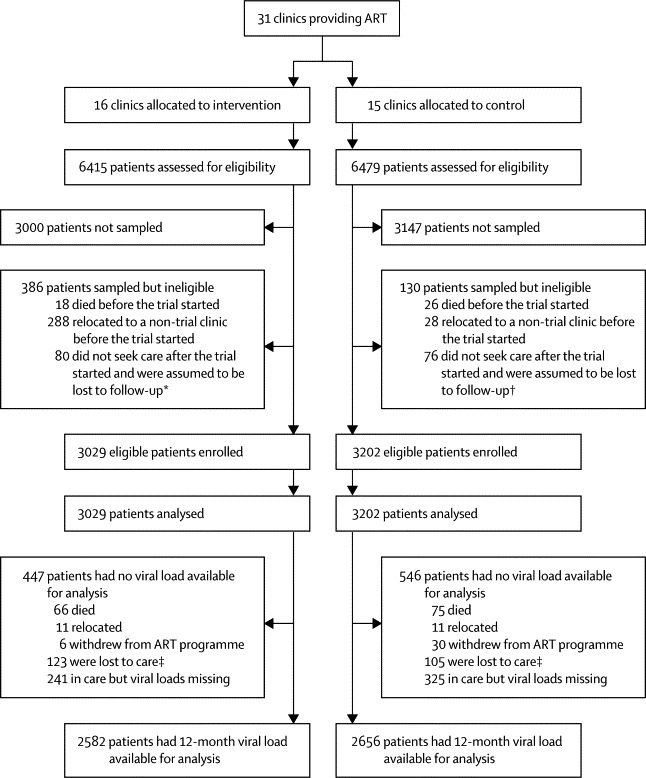
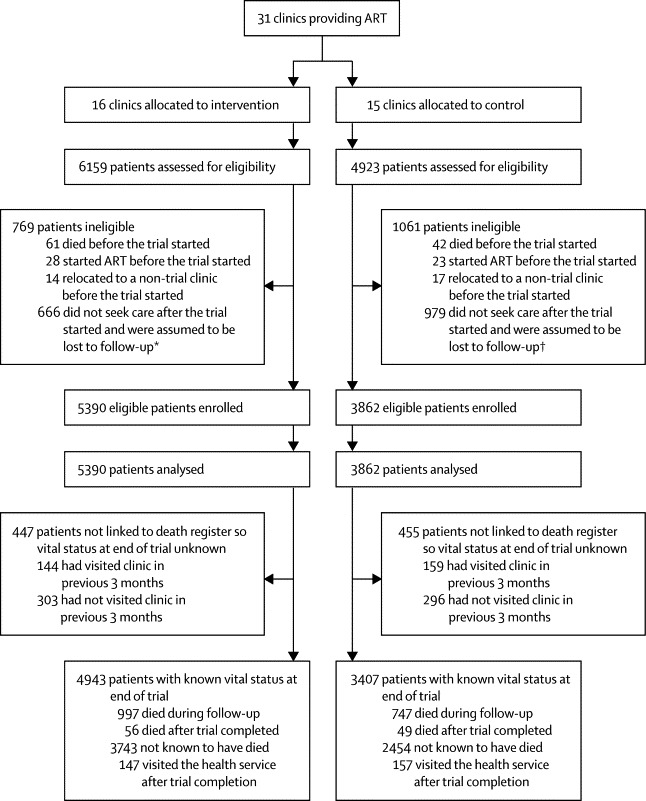
5390 patients in cohort 1 and 3029 in cohort 2 were in the intervention group, and 3862 in cohort 1 and 3202 in cohort 2 were in the control group. Median follow-up was 16·3 months (IQR 12·2-18·0) in cohort 1 and 18·0 months (18·0-18·0) in cohort 2. In cohort 1, 997 (20%) of 4943 patients analysed in the intervention group and 747 (19%) of 3862 in the control group with known vital status at the end of the trial had died. Time to death did not differ (hazard ratio [HR] 0·94, 95% CI 0·76-1·15). In a preplanned subgroup analysis of patients with baseline CD4 counts of 201-350 cells per μL, mortality was slightly lower in the intervention group than in the control group (0·73, 0·54-1.00; p=0·052), but it did not differ between groups in patients with baseline CD4 of 200 cells per μL or less (0·94, 0·76-1·15; p=0·577). In cohort 2, viral load suppression 12 months after enrolment was equivalent in intervention (2156 [71%] of 3029 patients) and control groups (2230 [70%] of 3202; risk difference 1·1%, 95% CI -2·4 to 4·6).
Expansion of primary-care nurses' roles to include ART initiation and represcription can be done safely, and improve health outcomes and quality of care, but might not reduce time to ART or mortality.
UK Medical Research Council, Development Cooperation Ireland, and Canadian International Development Agency.
将抗逆转录病毒疗法(ART)从医生转移到其他卫生工作者手中的任务转移具有强大的效果证据很少。我们旨在评估 Streamlining Tasks and Roles to Expand Treatment and Care for HIV(STRETCH)计划对死亡率、病毒抑制和其他健康结果和质量指标的影响,该计划为护士提供教育外展培训,以启动和重新开具 ART,并分散护理。
我们在南非进行了一项务实的、平行的、集群随机试验,时间为 2008 年 1 月 28 日至 2010 年 6 月 30 日。我们随机分配了 31 个初级保健 ART 诊所实施 STRETCH 计划(干预组)或继续进行标准护理(对照组)。随机化的比例取决于每个九个层次中的诊所数量。招募了两个队列:队列 1 中的合格患者为年龄≥16 岁、CD4 计数<350 个细胞/μL 且未接受 ART 的成年人;队列 2 中的成年人已经接受了至少 6 个月的 ART 治疗,并且在登记时正在接受治疗。队列 1 的主要结果是死亡时间(优势分析)。队列 2 的主要结果是在登记后 12 个月时病毒载量不可检测(<400 拷贝/ml)的比例(等效性分析,预设差异<6%)。患者和临床医生不能对组分配进行屏蔽。中期分析是盲法的,但在最终分析锁定数据库后,数据分析师无法屏蔽。分析均按意向治疗进行。该试验已注册,编号 ISRCTN46836853。
队列 1 中有 5390 名患者,队列 2 中有 3029 名患者在干预组,队列 1 中有 3862 名患者,队列 2 中有 3202 名患者在对照组。队列 1 的中位随访时间为 16.3 个月(IQR 12.2-18.0),队列 2 为 18.0 个月(18.0-18.0)。在队列 1 中,干预组 4943 名分析患者中已知死亡状态的患者有 997 人(20%),对照组 3862 名患者中有 747 人(19%)。死亡时间没有差异(风险比[HR]0.94,95%CI 0.76-1.15)。在基线 CD4 计数为 201-350 个细胞/μL 的患者的预先计划的亚组分析中,干预组的死亡率略低于对照组(0.73,0.54-1.00;p=0.052),但在基线 CD4 计数为 200 个细胞/μL 或更低的患者中,两组之间没有差异(0.94,0.76-1.15;p=0.577)。在队列 2 中,登记后 12 个月的病毒载量抑制在干预组(3029 名患者中的 2156 名,71%)和对照组(3202 名患者中的 2230 名,70%)中相当;风险差异为 1.1%,95%CI-2.4 至 4.6。
扩大初级保健护士的角色,包括启动和重新开具 ART,可以安全进行,并改善健康结果和护理质量,但可能不会缩短接受 ART 的时间或降低死亡率。
英国医学研究理事会、爱尔兰发展合作署和加拿大国际发展署。