Centre for Clinical Research, Uppsala University, Central Hospital, Västerås, Sweden.
Scand J Trauma Resusc Emerg Med. 2012 Aug 20;20:57. doi: 10.1186/1757-7241-20-57.
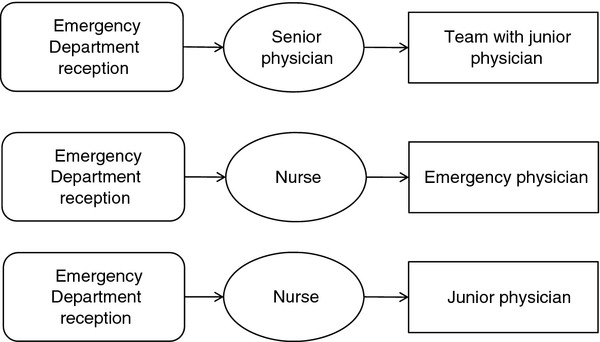
The management of emergency departments (EDs) principally involves maintaining effective patient flow and care. Different triage models are used today to achieve these two goals. The aim of this study was to compare the performance of different triage models used in three Swedish EDs. Using efficiency and quality indicators, we compared the following triage models: physician-led team triage, nurse first/emergency physician second, and nurse first/junior physician second.
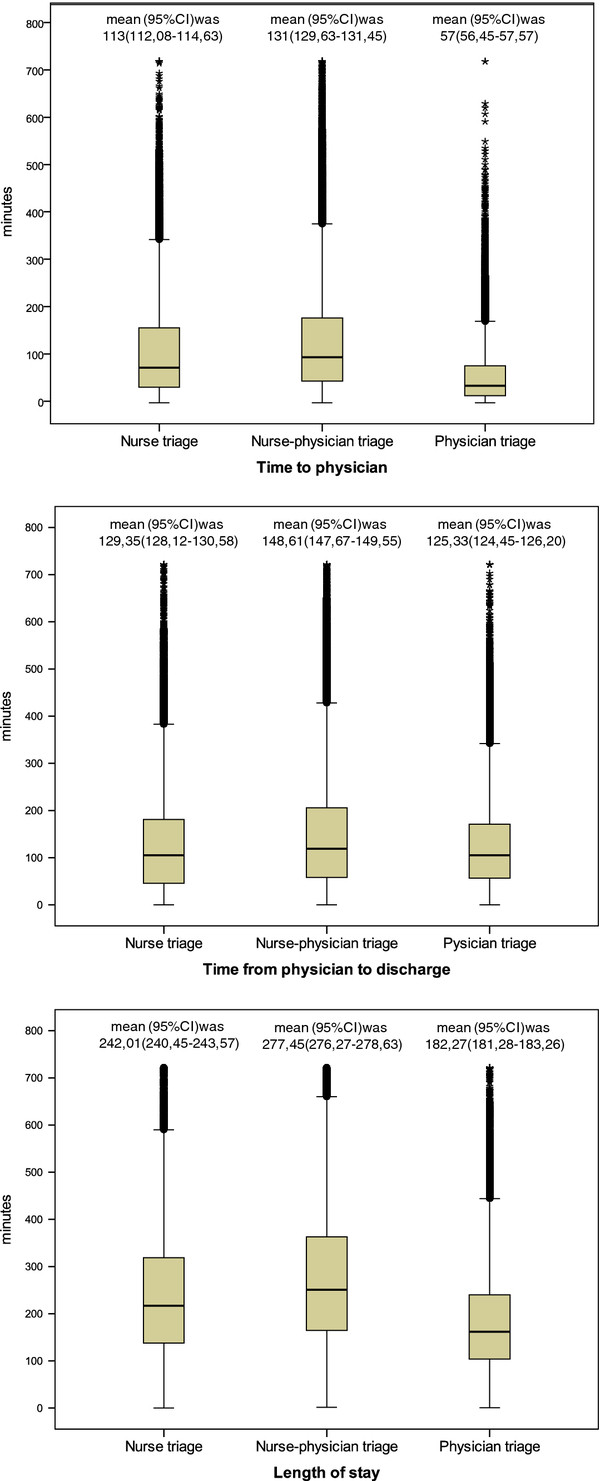
All data of patients arriving at the three EDs between 08:00- and 21:00 throughout 2008 were collected and merged into a database. The following efficiency indicators were measured: length of stay (LOS) including time to physician, time from physician to discharge, and 4-hour turnover rate. The following quality indicators were measured: rate of patients left before treatment was completed, unscheduled return within 24 and 72 hours, and mortality rate within 7 and 30 days.
Data from 147,579 patients were analysed. The median length of stay was 158 minutes for physician-led team triage, compared with 243 and 197 minutes for nurse/emergency physician and nurse/junior physician triage, respectively (p < 0.001). The rate of patients left before treatment was completed was 3.1% for physician-led team triage, 5.3% for nurse/emergency physician, and 9.6% for nurse/junior physician triage (p < 0.001). Further, the rates of unscheduled return within 24 hours were significantly lower for physician-led team triage, 1.0%, compared with 2.1%, and 2.5% for nurse/emergency physician, and nurse/junior physician, respectively (p < 0.001). The mortality rate within 7 days was 0.8% for physician-led team triage and 1.0% for the two other triage models (p < 0.001).
Physician-led team triage seemed advantageous, both expressed as efficiency and quality indicators, compared with the two other models.
急诊科(ED)的管理主要涉及保持有效的患者流程和护理。目前使用不同的分诊模型来实现这两个目标。本研究的目的是比较在瑞典三个急诊科使用的不同分诊模型的性能。使用效率和质量指标,我们比较了以下分诊模型:医生领导的团队分诊、护士首先/急诊医生其次和护士首先/初级医生其次。
收集了 2008 年每天 8:00 至 21:00 期间到达三个急诊科的所有患者的数据,并将其合并到一个数据库中。测量了以下效率指标:包括从医生到出院的时间,以及 4 小时周转率的停留时间(LOS)。测量了以下质量指标:治疗完成前离开的患者比例、24 小时和 72 小时内未计划返回的患者比例,以及 7 天和 30 天内的死亡率。
分析了 147579 名患者的数据。医生领导的团队分诊的中位停留时间为 158 分钟,而护士/急诊医生和护士/初级医生分诊的停留时间分别为 243 分钟和 197 分钟(p<0.001)。治疗完成前离开的患者比例为 3.1%的医生领导的团队分诊,5.3%的护士/急诊医生和 9.6%的护士/初级医生分诊(p<0.001)。此外,医生领导的团队分诊的 24 小时内未计划返回的比例明显较低,为 1.0%,而护士/急诊医生和护士/初级医生的比例分别为 2.1%和 2.5%(p<0.001)。7 天内的死亡率为 0.8%的医生领导的团队分诊和 1.0%的另外两种分诊模型(p<0.001)。
与另外两种模型相比,医生领导的团队分诊在效率和质量指标方面似乎具有优势。