Department of Anesthesiology, Division of Critical Care Medicine, Université Laval, Centre Hospitalier Affilié Universitaire de Québec, Enfant-Jésus Hospital, Québec City, QC, Canada G1J 1Z4.
BMJ. 2012 Aug 28;345:e5389. doi: 10.1136/bmj.e5389.
To evaluate the risk of postoperative bleeding and reintervention with the use of systemic steroids in patients undergoing tonsillectomy.
Systematic review and meta-analysis of randomised controlled trials.
Medline, Embase, Cochrane Library, Scopus, Web of Science, Intute, Biosis, OpenSIGLE, National Technical Information Service, and Google Scholar were searched. References from reviews identified in the search and from included studies were scanned.
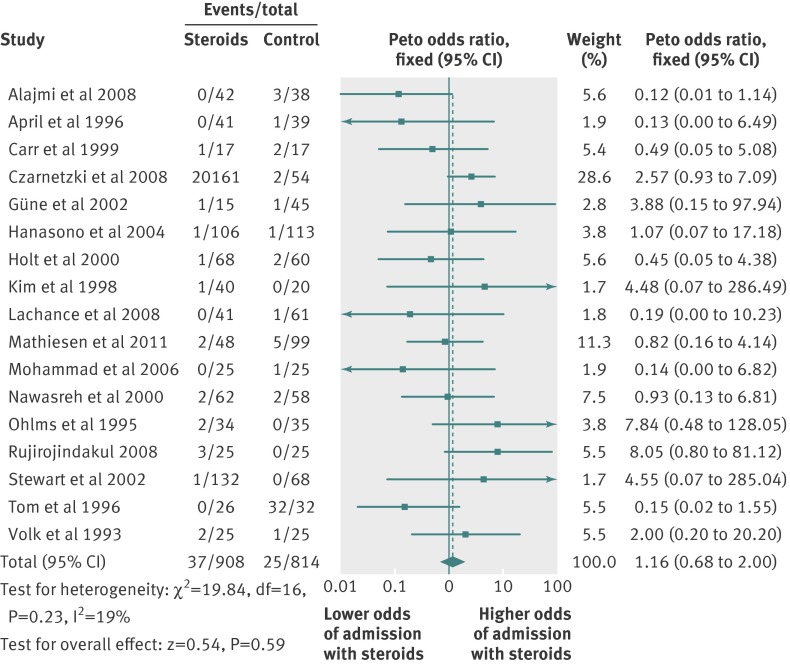
Randomised controlled trials comparing the administration of systemic steroids during tonsillectomy with any other comparator were eligible. Primary outcome was postoperative bleeding. Secondary outcomes were the rate of admission for a bleeding episode, reintervention for a bleeding episode, blood transfusion, and mortality.
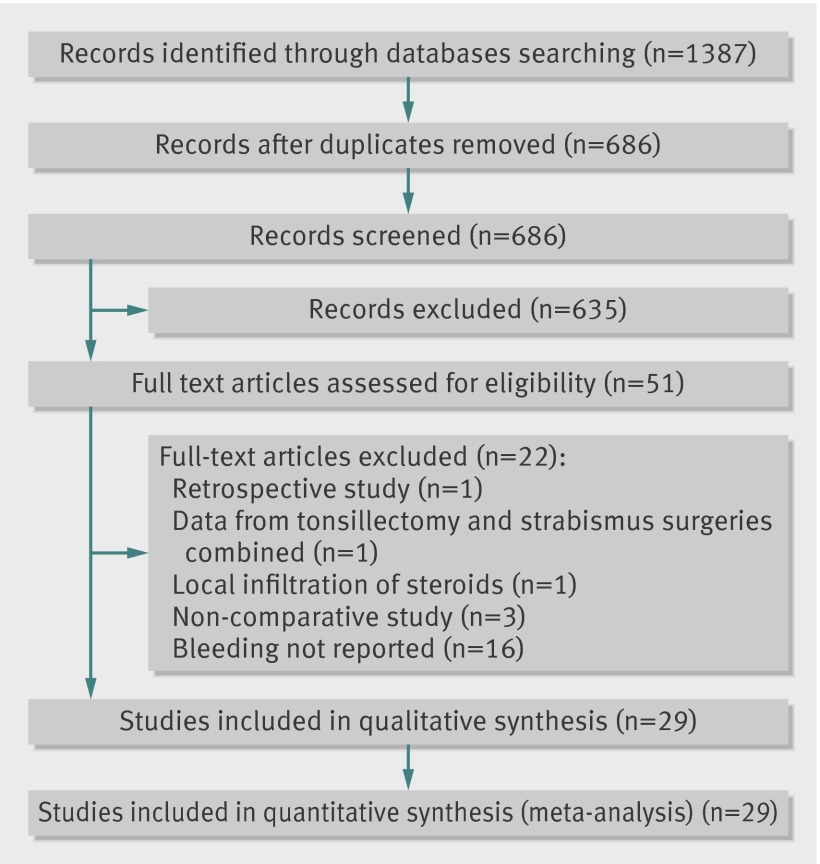
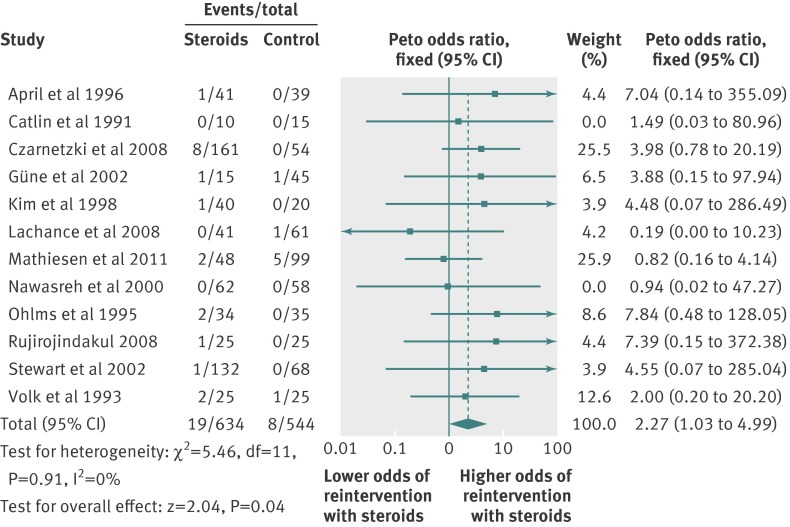
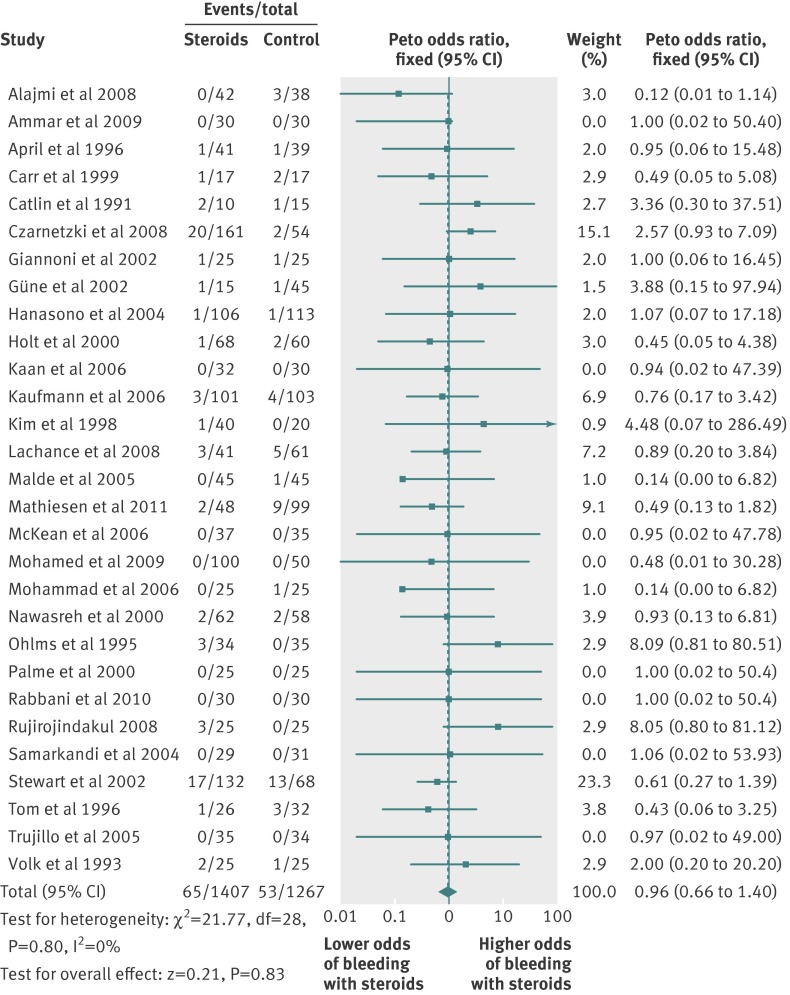
Of 1387 citations identified, 29 randomised controlled trials (n=2674) met all eligibility criteria. Seven studies presented a low risk of bias, but none was specifically designed to systematically identify postoperative bleeding. Administration of systemic steroids did not significantly increase the incidence of post-tonsillectomy bleeding (29 studies, n=2674 patients, odds ratio 0.96 (95% confidence interval 0.66 to 1.40), I²=0%). We observed a significant increase in the incidence of operative reinterventions for bleeding episodes in patients who received systemic steroids (12, n=1178, 2.27 (1.03 to 4.99), I²=0%). No deaths were reported. Sensitivity analyses were consistent with the findings.
Although systemic steroids do not appear to increase bleeding events after tonsillectomy, their use is associated with a raised incidence of operative reinterventions for bleeding episodes, which may be related to increased severity of bleeding events. Systemic steroids should be used with caution, and the risks and benefits weighed, for the prevention of postoperative nausea and vomiting after tonsillectomy before further research is performed to clarify their condition of use.
评估在扁桃体切除术中使用全身类固醇治疗患者术后出血和再次干预的风险。
系统评价和随机对照试验的荟萃分析。
检索了 Medline、Embase、Cochrane 图书馆、Scopus、Web of Science、Intute、Biosis、OpenSIGLE、美国国家技术信息服务局和 Google Scholar,并扫描了综述中确定的参考文献和纳入研究的参考文献。
比较扁桃体切除术中全身应用类固醇与任何其他对照药物的随机对照试验符合入选标准。主要结局是术后出血。次要结局是出血发作的住院率、出血发作的再次干预、输血和死亡率。
从 1387 篇引文中共纳入 29 项随机对照试验(n=2674),均符合所有入选标准。7 项研究的偏倚风险较低,但没有一项研究专门设计用于系统地识别术后出血。全身应用类固醇并不能显著增加扁桃体切除术后出血的发生率(29 项研究,n=2674 例患者,比值比 0.96(95%置信区间 0.66 至 1.40),I²=0%)。我们发现接受全身类固醇治疗的患者发生手术干预以治疗出血的发生率显著增加(12 项研究,n=1178 例患者,2.27(1.03 至 4.99),I²=0%)。没有报告死亡病例。敏感性分析结果与上述发现一致。
尽管全身类固醇似乎不会增加扁桃体切除术后出血事件的发生,但它们的使用与手术干预治疗出血的发生率增加有关,这可能与出血事件的严重程度增加有关。在进一步研究澄清其使用条件之前,应谨慎使用全身类固醇预防扁桃体切除术后恶心和呕吐,并权衡其风险和益处。