Epicentre, 8 rue Saint-Sabin, Paris, France.
Popul Health Metr. 2012 Sep 4;10(1):18. doi: 10.1186/1478-7954-10-18.
During 2010, a community-based, sentinel site prospective surveillance system measured mortality, acute malnutrition prevalence, and the coverage of a Médecins Sans Frontières (MSF) intervention in four sous-préfectures of Lobaye prefecture in southwestern Central African Republic. We describe this surveillance system and its evaluation.
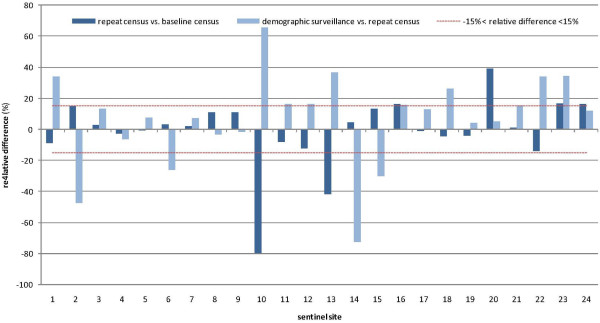
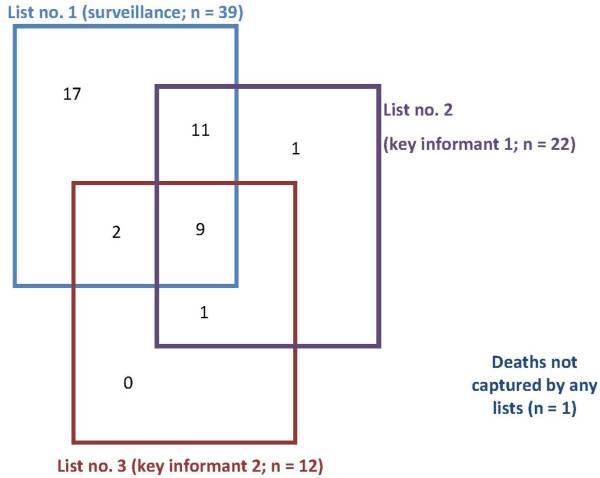
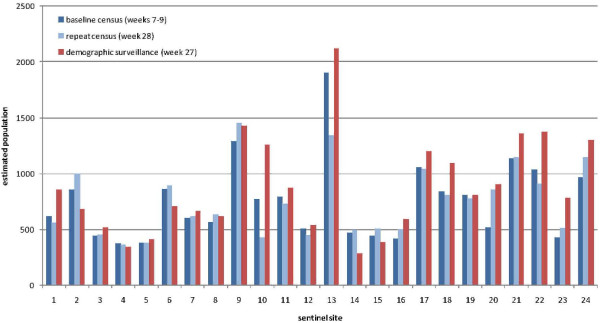
Within 24 randomly selected sentinel sites, home visitors performed a census, weekly demographic surveillance of births, deaths, and in- or out-migration, and weekly anthropometry on a sample of children. We evaluated the system through various methods including capture-recapture analysis and repeat census.
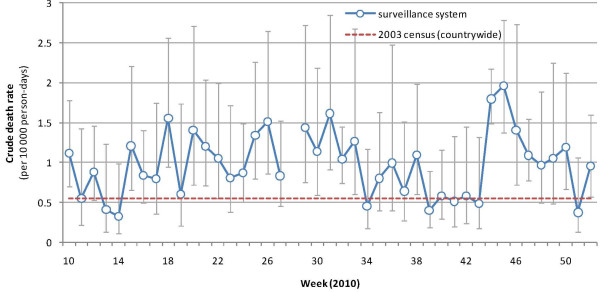
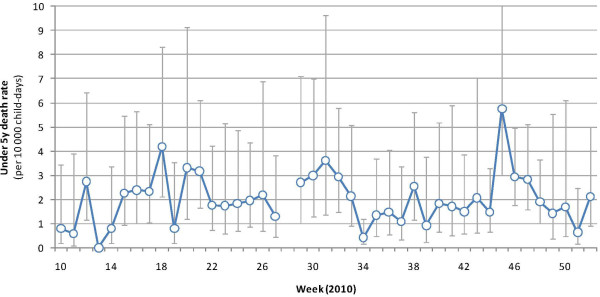
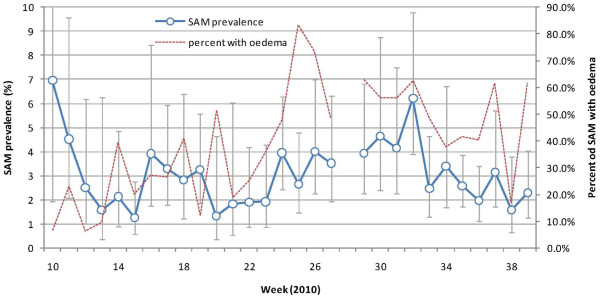
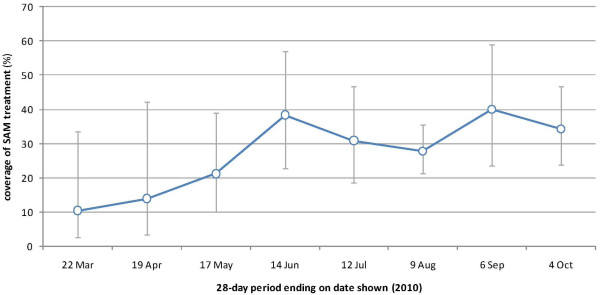
The system included 18,081 people at baseline. Over 32 weeks, the crude death rate was 1.0 (95% confidence interval [CI]: 0.8-1.2) deaths per 10,000 person-days (35 deaths per 1,000 person-years), with higher values during the rainy season. The under-5 death rate was approximately double. The prevalence of severe acute malnutrition (SAM) was 3.0% (95% CI: 2.3-4.0), almost half featuring kwashiorkor signs. The coverage of SAM treatment was 29.1%. The system detected >90% of deaths, and >90% of death reports appeared valid. However, demographic surveillance yielded discrepancies with the census and an implausible rate of population growth, while the predictive value of SAM classification was around 60%.
We found evidence of a chronic health crisis in this remote region. MSF's intervention coverage improved progressively. Mortality data appeared valid, but inaccuracies in population denominators and anthropometric measurements were noted. Similar systems could be implemented in other remote settings and acute emergencies, but with certain technical improvements.
2010 年期间,一个基于社区的哨点前瞻性监测系统测量了中非共和国西南部洛巴耶省四个专区的死亡率、急性营养不良流行率和无国界医生组织(MSF)干预措施的覆盖范围。我们描述了这个监测系统及其评估。
在 24 个随机选择的哨点中,家访员进行了一次人口普查,每周对出生、死亡和内外迁移进行人口监测,并对儿童样本进行每周人体测量。我们通过各种方法评估了该系统,包括捕获再捕获分析和重复人口普查。
该系统在基线时包括 18081 人。在 32 周内,粗死亡率为 1.0(95%置信区间[CI]:0.8-1.2)每 10000 人天死亡(每 1000 人年 35 人死亡),雨季时更高。5 岁以下儿童的死亡率大约是两倍。严重急性营养不良(SAM)的患病率为 3.0%(95%CI:2.3-4.0),近一半伴有夸希奥科营养不良的迹象。SAM 治疗的覆盖率为 29.1%。该系统检测到>90%的死亡病例,并且>90%的死亡报告似乎有效。然而,人口监测与人口普查存在差异,且人口增长率似乎不合理,而 SAM 分类的预测值约为 60%。
我们在这个偏远地区发现了慢性健康危机的证据。无国界医生组织的干预措施覆盖率逐步提高。死亡率数据似乎有效,但人口分母和人体测量值存在不准确。类似的系统可以在其他偏远地区和急性紧急情况下实施,但需要进行某些技术改进。