Department of Medicine, Fortis Escorts Hospital, Jaipur, Rajasthan, India.
PLoS One. 2012;7(8):e44098. doi: 10.1371/journal.pone.0044098. Epub 2012 Aug 29.
To determine correlation of multiple parameters of socioeconomic status with cardiovascular risk factors in India.
The study was performed at eleven cities using cluster sampling. Subjects (n = 6198, men 3426, women 2772) were evaluated for socioeconomic, demographic, biophysical and biochemical factors. They were classified into low, medium and high socioeconomic groups based on educational level (<10, 10-15 and >15 yr formal education), occupational class and socioeconomic scale. Risk factor differences were evaluated using multivariate logistic regression.
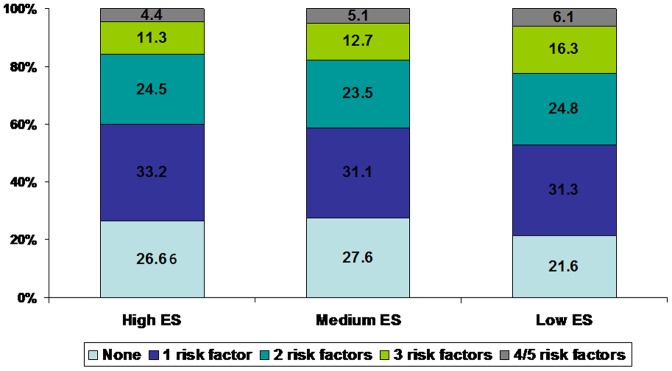
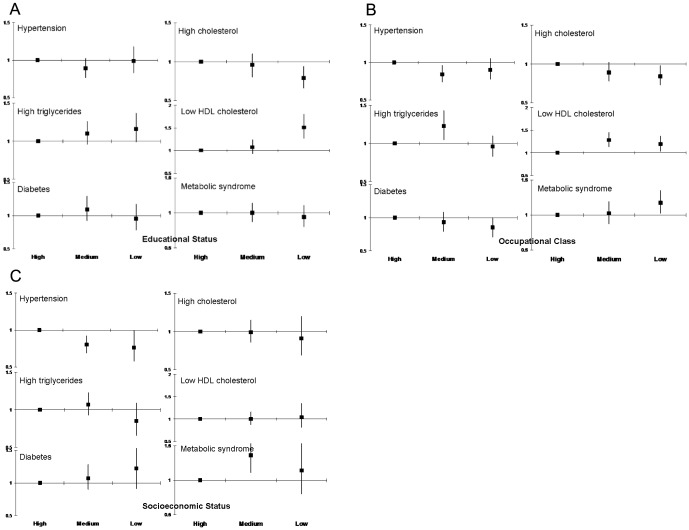
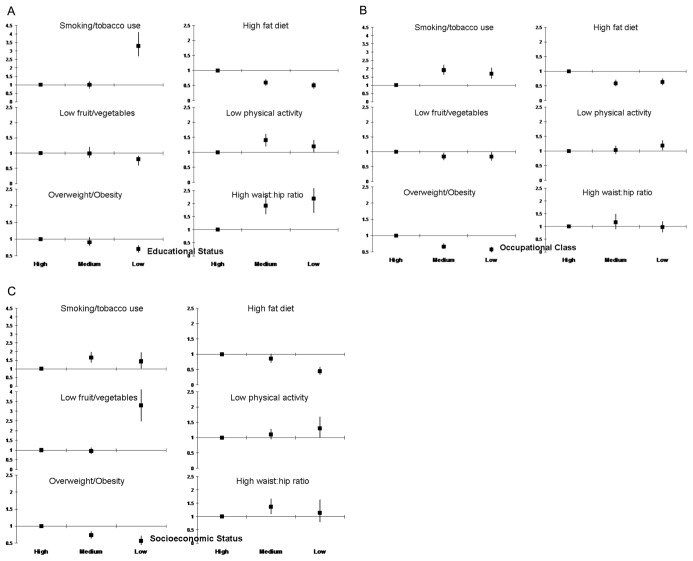
Age-adjusted prevalence (%) of risk factors in men and women was overweight or obesity in 41.1 and 45.2, obesity 8.3 and 15.8, high waist circumference 35.7 and 57.5, high waist-hip ratio 69.0 and 83.8, hypertension 32.5 and 30.4, hypercholesterolemia 24.8 and 25.3, low HDL cholesterol 34.1 and 35.1, high triglycerides 41.2 and 31.5, diabetes 16.7 and 14.4 and metabolic syndrome in 32.2 and 40.4 percent. Lifestyle factors were smoking 12.0 and 0.5, other tobacco use 12.7 and 6.3, high fat intake 51.2 and 48.2, low fruits/vegetables intake 25.3 and 28.9, and physical inactivity in 38.8 and 46.1%. Prevalence of > = 3 risk factors was significantly greater in low (28.0%) vs. middle (23.9%) or high (22.1%) educational groups (p<0.01). In low vs. high educational groups there was greater prevalence of high waist-hip ratio (odds ratio 2.18, confidence interval 1.65-2.71), low HDL cholesterol (1.51, 1.27-1.80), hypertriglyceridemia (1.16, 0.99-1.37), smoking/tobacco use (3.27, 2.66-4.01), and low physical activity (1.15, 0.97-1.37); and lower prevalence of high fat diet (0.47, 0.38-0.57),overweight/obesity (0.68, 0.58-0.80) and hypercholesterolemia (0.79, 0.66-0.94). Similar associations were observed with occupational and socioeconomic status.
Low educational, occupational and socioeconomic status Asian Indians have greater prevalence of truncal obesity, low HDL cholesterol, hypertriglyceridemia, smoking or tobacco use and low physical activity and clustering of > = 3 major cardiovascular risk factors.
为了确定印度社会经济地位的多个参数与心血管危险因素之间的相关性。
该研究在 11 个城市使用聚类抽样进行。对 6198 名受试者(男性 3426 名,女性 2772 名)进行了社会经济、人口统计学、生物物理和生物化学因素的评估。根据教育程度(<10 年、10-15 年和>15 年正规教育)、职业阶层和社会经济状况将他们分为低、中、高社会经济组。使用多变量逻辑回归评估危险因素差异。
男性和女性年龄调整后的风险因素患病率(%)分别为超重或肥胖 41.1 和 45.2,肥胖 8.3 和 15.8,高腰围 35.7 和 57.5,高腰臀比 69.0 和 83.8,高血压 32.5 和 30.4,高胆固醇血症 24.8 和 25.3,低高密度脂蛋白胆固醇 34.1 和 35.1,高甘油三酯 41.2 和 31.5,糖尿病 16.7 和 14.4,代谢综合征 32.2 和 40.4%。生活方式因素为吸烟 12.0 和 0.5,其他烟草使用 12.7 和 6.3,高脂肪摄入 51.2 和 48.2,低水果/蔬菜摄入 25.3 和 28.9,38.8 和 46.1%的人缺乏体育锻炼。低(28.0%)与中(23.9%)或高(22.1%)教育组相比,> = 3 个危险因素的患病率明显更高(p<0.01)。与高教育组相比,低教育组的高腰臀比(比值比 2.18,置信区间 1.65-2.71)、低高密度脂蛋白胆固醇(1.51,1.27-1.80)、高甘油三酯血症(1.16,0.99-1.37)、吸烟/烟草使用(3.27,2.66-4.01)和低体力活动(1.15,0.97-1.37)的患病率更高,而高脂肪饮食(0.47,0.38-0.57)、超重/肥胖(0.68,0.58-0.80)和高胆固醇血症(0.79,0.66-0.94)的患病率较低。职业和社会经济地位也存在类似的关联。
亚洲低教育程度、职业和社会经济地位的印度人存在更大的躯干肥胖、低高密度脂蛋白胆固醇、高甘油三酯血症、吸烟或烟草使用以及低体力活动和> = 3 个主要心血管危险因素聚集的风险。