Department of Radiation Oncology,1 Washington University School of Medicine, St. Louis, MO, USA.
J Appl Clin Med Phys. 2012 Sep 6;13(5):3837. doi: 10.1120/jacmp.v13i5.3837.
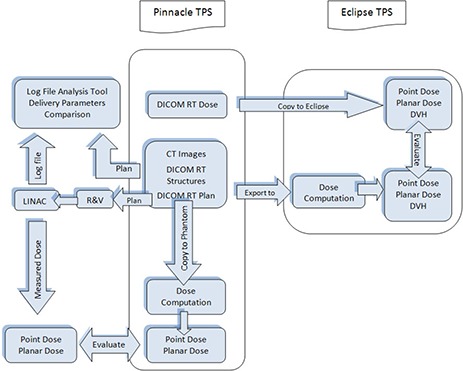
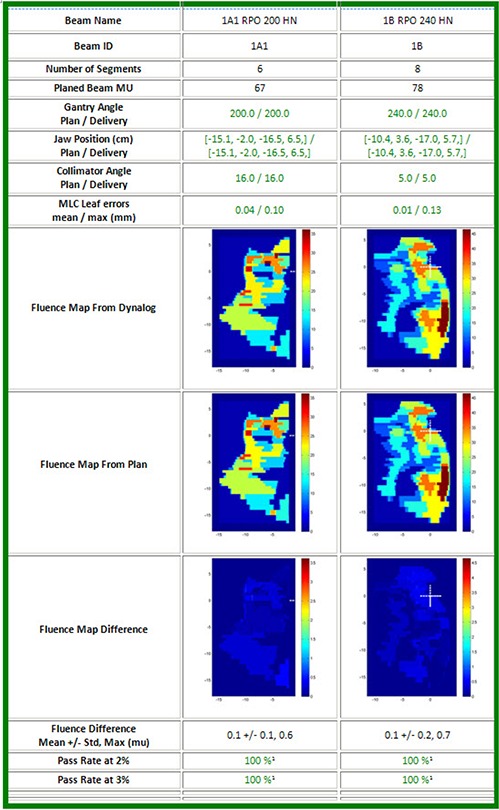
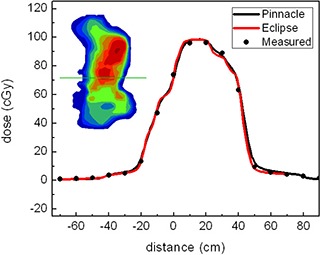
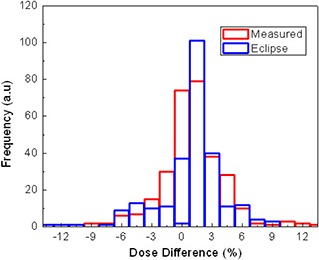
Experimental methods are commonly used for patient-specific IMRT delivery verification. There are a variety of IMRT QA techniques which have been proposed and clinically used with a common understanding that not one single method can detect all possible errors. The aim of this work was to compare the efficiency and effectiveness of independent dose calculation followed by machine log file analysis to conventional measurement-based methods in detecting errors in IMRT delivery. Sixteen IMRT treatment plans (5 head-and-neck, 3 rectum, 3 breast, and 5 prostate plans) created with a commercial treatment planning system (TPS) were recalculated on a QA phantom. All treatment plans underwent ion chamber (IC) and 2D diode array measurements. The same set of plans was also recomputed with another commercial treatment planning system and the two sets of calculations were compared. The deviations between dosimetric measurements and independent dose calculation were evaluated. The comparisons included evaluations of DVHs and point doses calculated by the two TPS systems. Machine log files were captured during pretreatment composite point dose measurements and analyzed to verify data transfer and performance of the delivery machine. Average deviation between IC measurements and point dose calculations with the two TPSs for head-and-neck plans were 1.2 ± 1.3% and 1.4 ± 1.6%, respectively. For 2D diode array measurements, the mean gamma value with 3% dose difference and 3 mm distance-to-agreement was within 1.5% for 13 of 16 plans. The mean 3D dose differences calculated from two TPSs were within 3% for head-and-neck cases and within 2% for other plans. The machine log file analysis showed that the gantry angle, jaw position, collimator angle, and MUs were consistent as planned, and maximal MLC position error was less than 0.5 mm. The independent dose calculation followed by the machine log analysis takes an average 47 ± 6 minutes, while the experimental approach (using IC and 2D diode array measurements) takes an average about 2 hours in our clinic. Independent dose calculation followed by machine log file analysis can be a reliable tool to verify IMRT treatments. Additionally, independent dose calculations have the potential to identify several problems (heterogeneity calculations, data corruptions, system failures) with the primary TPS, which generally are not identifiable with a measurement-based approach. Additionally, machine log file analysis can identify many problems (gantry, collimator, jaw setting) which also may not be detected with a measurement-based approach. Machine log file analysis could also detect performance problems for individual MLC leaves which could be masked in the analysis of a measured fluence.
实验方法常用于个体化调强放疗的验证。目前已经提出了多种调强放疗质量保证技术,临床应用时的共识是,没有一种单一的方法可以检测到所有可能的误差。本研究旨在比较独立剂量计算后结合机器日志文件分析与传统基于测量的方法在检测调强放疗中误差的效率和有效性。16 个调强治疗计划(5 个头颈部、3 个直肠、3 个乳腺和 5 个前列腺计划)由商业治疗计划系统(TPS)创建,并在 QA 体模上重新计算。所有治疗计划均进行电离室(IC)和 2D 二极管阵列测量。同一组计划还使用另一个商业治疗计划系统重新计算,并比较了两种计算结果。评估剂量测量值与独立剂量计算之间的偏差。比较包括两个 TPS 系统计算的剂量学体积直方图(DVH)和点剂量。在预治疗复合点剂量测量期间捕获机器日志文件,并进行分析以验证数据传输和输送机器的性能。对于头颈部计划,IC 测量值与两个 TPS 点剂量计算之间的平均偏差分别为 1.2%±1.3%和 1.4%±1.6%。对于 2D 二极管阵列测量,16 个计划中有 13 个的 3%剂量差异和 3mm 距离一致性的平均伽马值在 1.5%以内。从两个 TPS 计算的平均 3D 剂量差异对头颈部病例在 3%以内,其他计划在 2%以内。机器日志文件分析表明,准直器角度、机架角度、准直器角度和 MU 与计划一致,最大叶片位置误差小于 0.5mm。独立剂量计算后结合机器日志分析平均需要 47±6 分钟,而我们临床使用 IC 和 2D 二极管阵列测量的实验方法平均需要 2 小时左右。独立剂量计算后结合机器日志文件分析可以成为验证调强放疗的可靠工具。此外,独立剂量计算有可能识别主要 TPS 中的一些问题(不均匀性计算、数据损坏、系统故障),而基于测量的方法通常无法识别这些问题。此外,机器日志文件分析还可以识别许多问题(机架、准直器、机架设置),这些问题也可能无法通过基于测量的方法检测到。机器日志文件分析还可以检测单个叶片的性能问题,而在测量的通量分析中可能会掩盖这些问题。