Department of Clinical Pharmacology, Medical University of Vienna, Waehringer Guertel 18-20, 1090 Vienna, Austria.
Curr Opin Pharmacol. 2013 Feb;13(1):36-42. doi: 10.1016/j.coph.2012.09.003. Epub 2012 Sep 23.
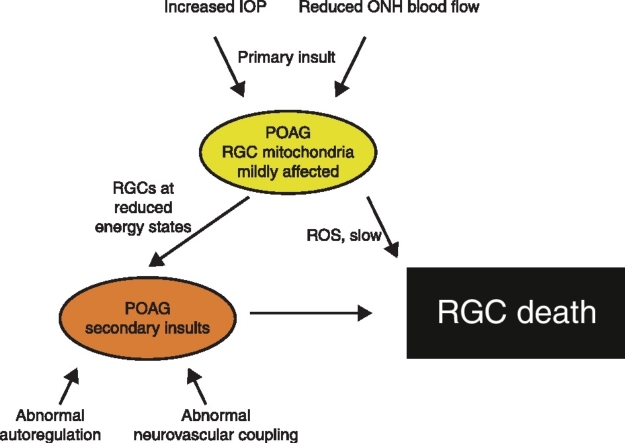
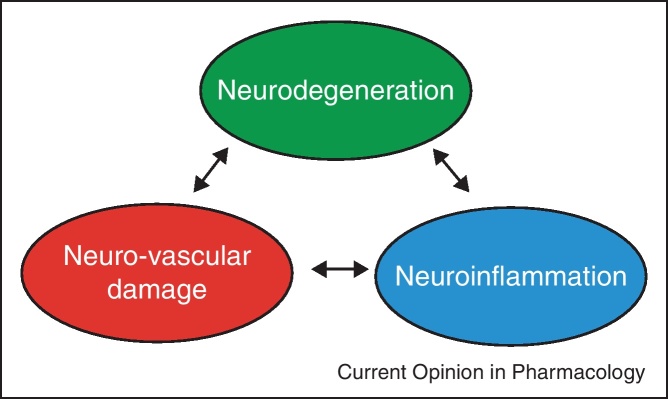
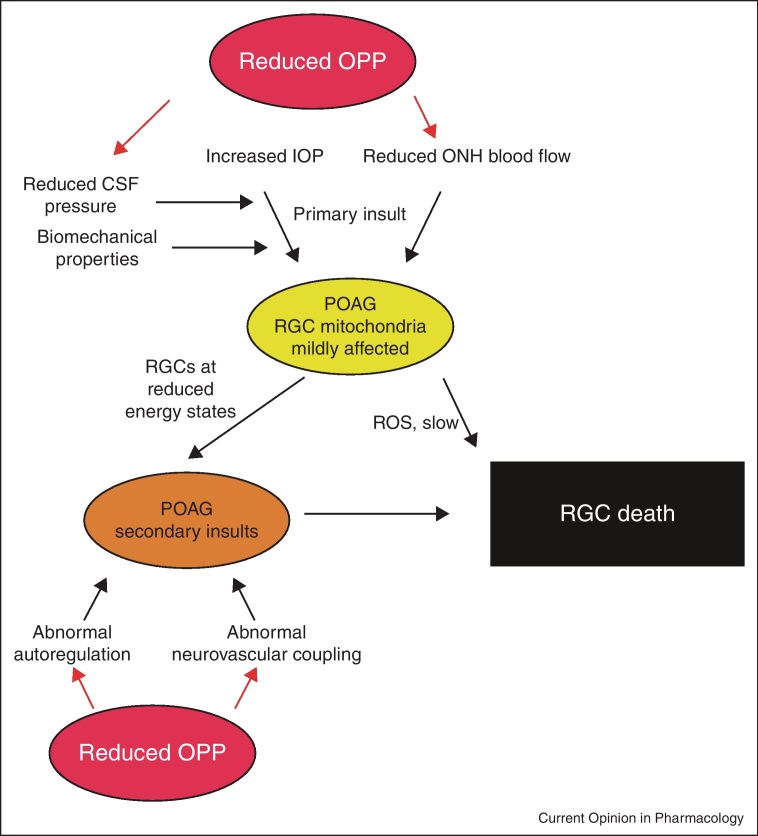
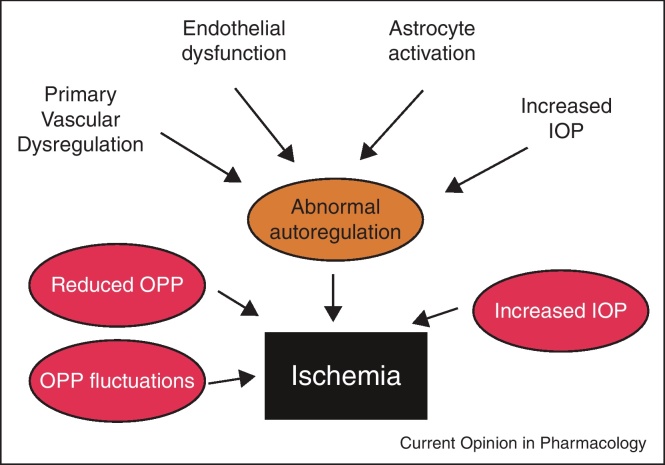
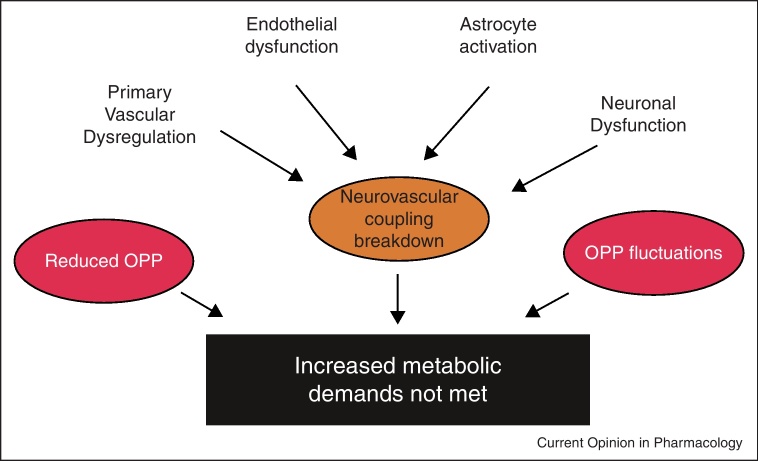
Glaucoma is a progressive optic neuropathy of unknown origin. It has been hypothesized that a vascular component is involved in glaucoma pathophysiology. This hypothesis has gained support from studies showing that reduced ocular perfusion pressure is a risk factor for the disease. The exact nature of the involvement is, however, still a matter of debate. Based on recent evidence we propose a model including primary and secondary insults in glaucoma. The primary insult appears to happen at the optic nerve head. Increased intraocular pressure and ischemia at the post-laminar optic nerve head affects retinal ganglion cell axons. Modulating factors are the biomechanical properties of the tissues and cerebrospinal fluid pressure. After this primary insult retinal ganglion cells function at a reduced energy level and are sensitive to secondary insults. These secondary insults may happen if ocular perfusion pressure falls below the lower limit of autoregulation or if neurovascular coupling fails. Evidence for both faulty autoregulation and reduced hyperemic response to neuronal stimulation has been provided in glaucoma patients. The mechanisms appear to involve vascular endothelial dysfunction and impaired astrocyte-vessel signaling. A more detailed understanding of these pathways is required to direct neuroprotective strategies via the neurovascular pathway.
青光眼是一种不明原因的进行性视神经病变。有人假设血管成分参与了青光眼的病理生理学。这一假设得到了一些研究的支持,这些研究表明,眼灌注压降低是该病的一个风险因素。然而,确切的参与性质仍存在争议。基于最近的证据,我们提出了一个包括青光眼原发性和继发性损伤的模型。原发性损伤似乎发生在视神经头部。眼内压升高和视盘后层缺血会影响视网膜神经节细胞轴突。调节因素是组织的生物力学特性和脑脊液压力。在这种原发性损伤之后,视网膜神经节细胞的功能处于能量降低的状态,并容易受到继发性损伤的影响。如果眼灌注压低于自动调节的下限,或者神经血管耦合失败,就可能发生这些继发性损伤。青光眼患者的证据表明,自动调节功能障碍和神经元刺激的高反应性降低都可能发生。这些机制似乎涉及血管内皮功能障碍和星形胶质细胞-血管信号传递受损。需要更详细地了解这些途径,以便通过神经血管途径指导神经保护策略。