The FOxTROT Trial, Birmingham Clinical Trials Unit, Robert Aitken Institute, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK.
Lancet Oncol. 2012 Nov;13(11):1152-60. doi: 10.1016/S1470-2045(12)70348-0. Epub 2012 Sep 25.
Preoperative (neoadjuvant) chemotherapy and radiotherapy are more effective than similar postoperative treatment for oesophageal, gastric, and rectal cancers, perhaps because of more effective micrometastasis eradication and reduced risk of incomplete excision and tumour cell shedding during surgery. The FOxTROT trial aims to investigate the feasibility, safety, and efficacy of preoperative chemotherapy for colon cancer.
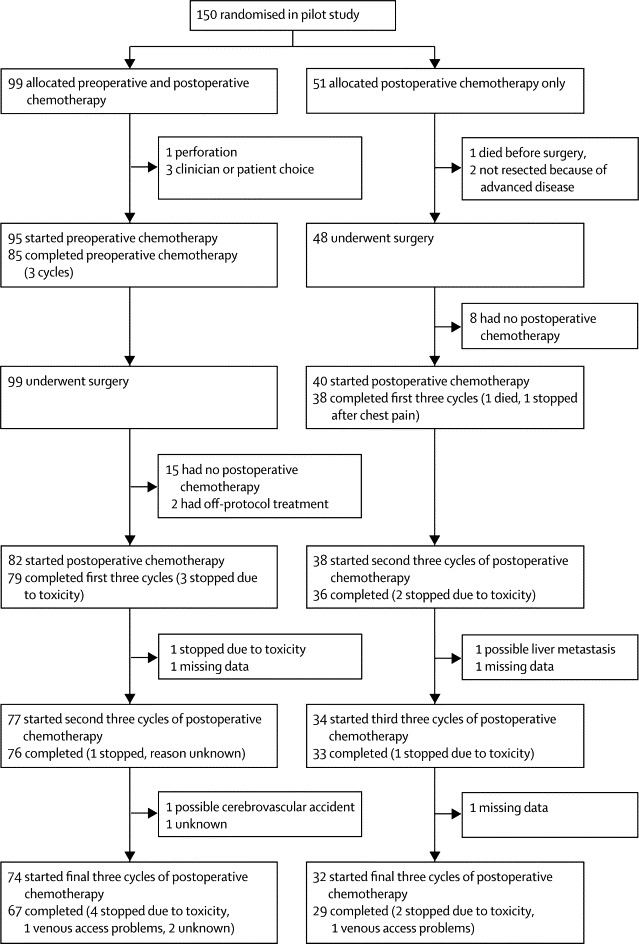
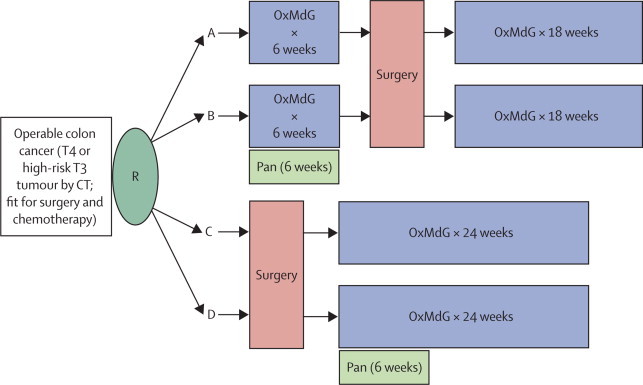
In the pilot stage of this randomised controlled trial, 150 patients with radiologically staged locally advanced (T3 with ≥5 mm invasion beyond the muscularis propria or T4) tumours from 35 UK centres were randomly assigned (2:1) to preoperative (three cycles of OxMdG [oxaliplatin 85 mg/m(2), l-folinic acid 175 mg, fluorouracil 400 mg/m(2) bolus, then 2400 mg/m(2) by 46 h infusion] repeated at 2-weekly intervals followed by surgery and a further nine cycles of OxMdG) or standard postoperative chemotherapy (12 cycles of OxMdG). Patients with KRAS wild-type tumours were randomly assigned (1:1) to receive panitumumab (6 mg/kg; every 2 weeks with the first 6 weeks of chemotherapy) or not. Treatment allocation was through a central randomisation service using a minimised randomisation procedure including age, radiological T and N stage, site of tumour, and presence of defunctioning colostomy as stratification variables. Primary outcome measures of the pilot phase were feasibility, safety, and tolerance of preoperative therapy, and accuracy of radiological staging. Analysis was by intention to treat. This trial is registered, number ISRCTN 87163246.
96% (95 of 99) of patients started and 89% (85 of 95) completed preoperative chemotherapy with grade 3-4 gastrointestinal toxicity in 7% (seven of 94) of patients. All 99 tumours in the preoperative group were resected, with no significant differences in postoperative morbidity between the preoperative and control groups: 14% (14 of 99) versus 12% (six of 51) had complications prolonging hospital stay (p=0·81). 98% (50 of 51) of postoperative chemotherapy patients had T3 or more advanced tumours confirmed at post-resection pathology compared with 91% (90 of 99) of patients following preoperative chemotherapy (p=0·10). Preoperative therapy resulted in significant downstaging of TNM5 compared with the postoperative group (p=0·04), including two pathological complete responses, apical node involvement (1% [one of 98] vs 20% [ten of 50], p<0·0001), resection margin involvement (4% [four of 99] vs 20% [ten of 50], p=0·002), and blinded centrally scored tumour regression grading: 31% (29 of 94) vs 2% (one of 46) moderate or greater regression (p=0·0001).
Preoperative chemotherapy for radiologically staged, locally advanced operable primary colon cancer is feasible with acceptable toxicity and perioperative morbidity. Proceeding to the phase 3 trial, to establish whether the encouraging pathological responses seen with preoperative therapy translates into improved long-term oncological outcome, is appropriate.
Cancer Research UK.
术前(新辅助)化疗和放疗比类似的术后治疗对食管、胃和直肠癌症更有效,这可能是因为在手术过程中更有效地清除微转移,降低不完全切除和肿瘤细胞脱落的风险。FOxTROT 试验旨在研究术前化疗治疗结肠癌的可行性、安全性和疗效。
在这项随机对照试验的试点阶段,来自英国 35 个中心的 150 名经影像学分期为局部晚期(T3 期,固有肌层浸润≥5mm 或 T4 期)的患者被随机分配(2:1)接受术前治疗(3 个周期 OxMdG [奥沙利铂 85mg/m²,亚叶酸 175mg,氟尿嘧啶 400mg/m² 推注,然后 2400mg/m² 持续输注],每 2 周重复一次,然后手术,再进行 9 个周期 OxMdG)或标准术后化疗(12 个周期 OxMdG)。KRAS 野生型肿瘤患者被随机分配(1:1)接受帕尼单抗(6mg/kg;每 2 周一次,前 6 周化疗)或不接受。通过中央随机化服务进行治疗分配,使用最小化随机化程序,包括年龄、影像学 T 和 N 分期、肿瘤部位和预防性结肠造口术的存在作为分层变量。试点阶段的主要结果测量是术前治疗的可行性、安全性和耐受性,以及影像学分期的准确性。分析是意向治疗。这项试验在 ClinicalTrials.gov 注册,编号为 ISRCTN87163246。
96%(99 例中的 99 例)的患者开始接受术前治疗,89%(95 例中的 85 例)完成了治疗,7%(94 例中的 7 例)出现 3-4 级胃肠道毒性。术前组的所有 99 个肿瘤均被切除,术前组和对照组术后发病率无显著差异:14%(99 例中的 14 例)与 12%(51 例中的 6 例)发生延长住院时间的并发症(p=0.81)。98%(51 例中的 50 例)的术后化疗患者在术后病理检查中发现 T3 期或更晚期肿瘤,而术前化疗组为 91%(99 例中的 90 例)(p=0.10)。与术后组相比,术前治疗导致 TNM5 显著降期(p=0.04),包括 2 例病理完全缓解、顶端淋巴结受累(1%[98 例中的 1 例] vs 20%[50 例中的 10 例],p<0.0001)、切缘受累(4%[99 例中的 4 例] vs 20%[50 例中的 10 例],p=0.002)和盲法中央评分的肿瘤消退分级:31%(94 例中的 29 例)vs 2%(46 例中的 1 例)中度或更显著消退(p=0.0001)。
对影像学分期为局部晚期、可手术的原发性结肠癌进行术前化疗是可行的,具有可接受的毒性和围手术期发病率。进行 3 期试验以确定术前治疗中观察到的令人鼓舞的病理反应是否转化为改善长期肿瘤学结局是合适的。
英国癌症研究中心。