Centre for International Health and Development, UCL Institute of Child Health, London, United Kingdom.
PLoS Med. 2012;9(10):e1001320. doi: 10.1371/journal.pmed.1001320. Epub 2012 Oct 2.
Households from vulnerable groups experiencing epidemiological transitions are known to be affected concomitantly by under-nutrition and obesity. Yet, it is unknown to what extent this double burden affects refugee populations dependent on food assistance. We assessed the double burden of malnutrition among Western Sahara refugees living in a protracted emergency.
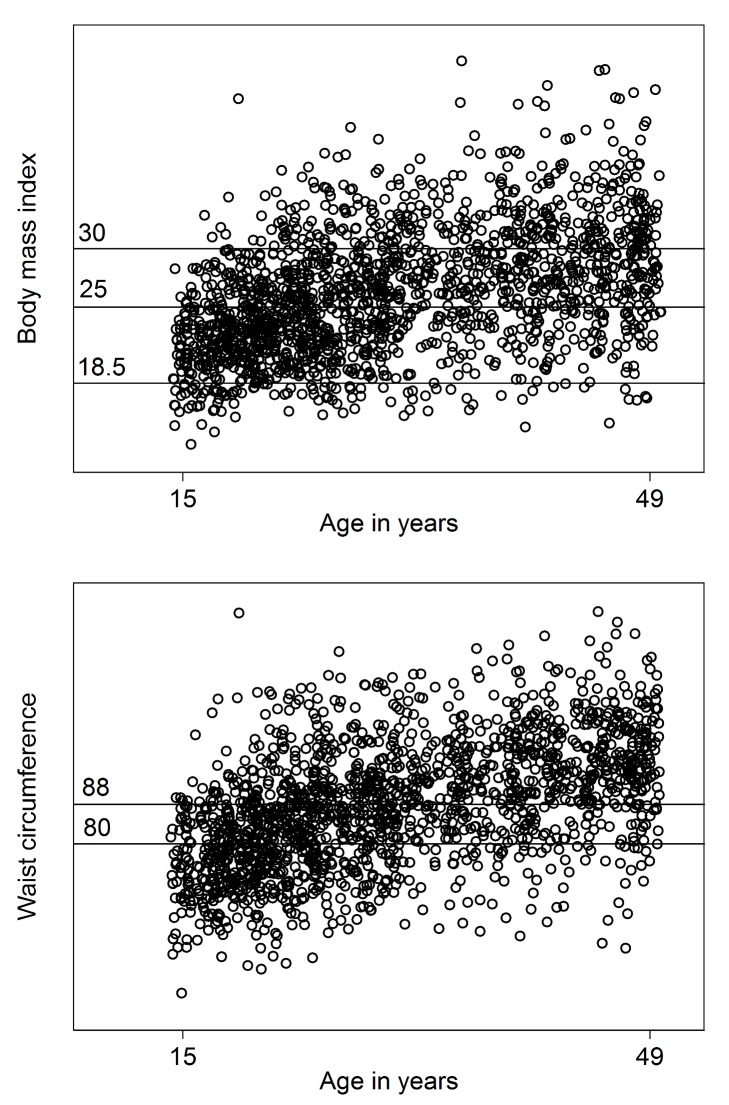
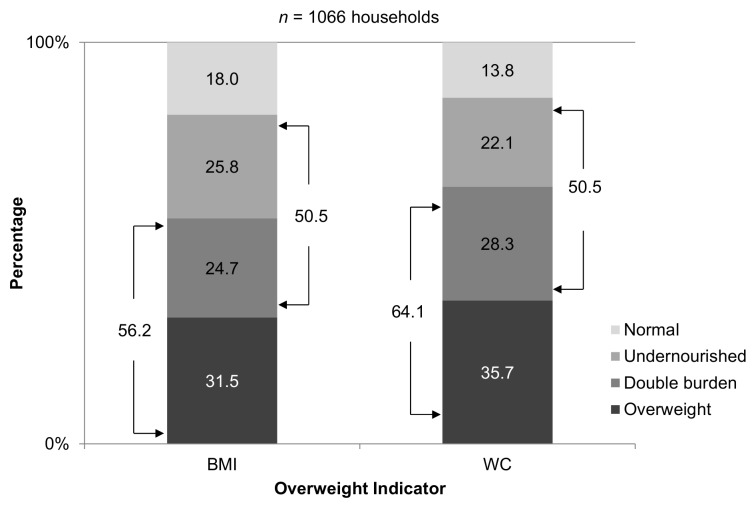
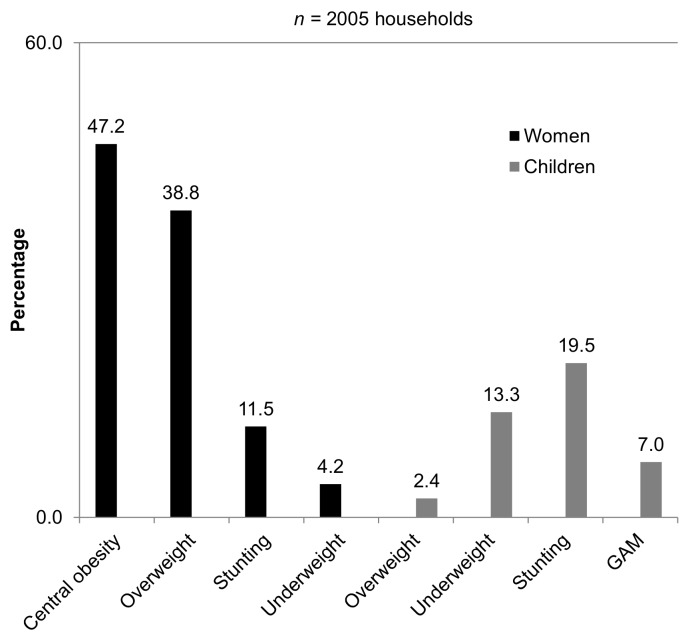
We implemented a stratified nutrition survey in October-November 2010 in the four Western Sahara refugee camps in Algeria. We sampled 2,005 households, collecting anthropometric measurements (weight, height, and waist circumference) in 1,608 children (6-59 mo) and 1,781 women (15-49 y). We estimated the prevalence of global acute malnutrition (GAM), stunting, underweight, and overweight in children; and stunting, underweight, overweight, and central obesity in women. To assess the burden of malnutrition within households, households were first classified according to the presence of each type of malnutrition. Households were then classified as undernourished, overweight, or affected by the double burden if they presented members with under-nutrition, overweight, or both, respectively. The prevalence of GAM in children was 9.1%, 29.1% were stunted, 18.6% were underweight, and 2.4% were overweight; among the women, 14.8% were stunted, 53.7% were overweight or obese, and 71.4% had central obesity. Central obesity (47.2%) and overweight (38.8%) in women affected a higher proportion of households than did GAM (7.0%), stunting (19.5%), or underweight (13.3%) in children. Overall, households classified as overweight (31.5%) were most common, followed by undernourished (25.8%), and then double burden-affected (24.7%).
The double burden of obesity and under-nutrition is highly prevalent in households among Western Sahara refugees. The results highlight the need to focus more attention on non-communicable diseases in this population and balance obesity prevention and management with interventions to tackle under-nutrition. Please see later in the article for the Editors' Summary.
弱势群体家庭在经历流行病学转变的同时,往往受到营养不良和肥胖的双重影响。然而,难民群体在多大程度上受到食品援助的影响,目前还不得而知。我们评估了居住在长期紧急情况中的西撒哈拉难民中营养不良的双重负担。
我们于 2010 年 10 月至 11 月在阿尔及利亚的四个西撒哈拉难民营中实施了一项分层营养调查。我们抽取了 2005 户家庭,在 1608 名 6-59 月龄儿童和 1781 名 15-49 岁妇女中收集了人体测量数据(体重、身高和腰围)。我们估计了儿童中全球急性营养不良(GAM)、发育迟缓、体重不足和超重的患病率;以及妇女中发育迟缓、体重不足、超重和中心性肥胖的患病率。为了评估家庭内营养不良的负担,首先根据每种营养不良的存在情况对家庭进行分类。如果家庭有成员存在营养不良、超重或两者兼有,则分别将其归类为营养不足、超重或受双重负担影响。儿童中 GAM 的患病率为 9.1%,29.1%发育迟缓,18.6%体重不足,2.4%超重;妇女中,14.8%发育迟缓,53.7%超重或肥胖,71.4%中心性肥胖。妇女中中心性肥胖(47.2%)和超重(38.8%)比儿童中 GAM(7.0%)、发育迟缓(19.5%)或体重不足(13.3%)更影响家庭比例。总体而言,超重(31.5%)的家庭最常见,其次是营养不足(25.8%),然后是受双重负担影响(24.7%)。
肥胖和营养不良的双重负担在西撒哈拉难民家庭中非常普遍。研究结果强调,需要更加关注这一人群中的非传染性疾病,并在预防和管理肥胖的同时,平衡干预措施以解决营养不良问题。请在文章后面查看编辑摘要。