Wells Diana L, Swanson Joseph M, Wood G Christopher, Magnotti Louis J, Boucher Bradley A, Croce Martin A, Harrison Charles G, Muhlbauer Michael S, Fabian Timothy C
Crit Care. 2012 Oct 15;16(5):R193. doi: 10.1186/cc11678.
Limited data suggest mild hypernatremia may be related to lower intracranial pressure (ICP) in patients with traumatic brain injury (TBI). The practice at the study center has been to use hypertonic saline (HTS) to generate a targeted serum sodium of 145 to 155 mEq/l in patients with TBI. The purpose of this study was to determine the relationship between serum sodium values and ICP, and to evaluate the acute effect of HTS on ICP.
A retrospective review of patients who were admitted to the trauma ICU for TBI, had an ICP monitor placed, and received at least one dose of HTS between January 2006 and March 2011 was performed. Data were collected for up to 120 hours after ICP monitor placement. The primary outcome was the relationship between serum sodium and maximum ICP. Secondary outcomes were the relationship between serum sodium and the mean number of daily interventions for ICP control, and the acute effect of HTS on ICP during the 6 hours after each dose. Linear regression was used to analyze the primary outcome. Analysis of variance on ranks and repeated measures analysis of variance were used to evaluate the number of interventions and the acute effect of HTS on ICP, respectively.
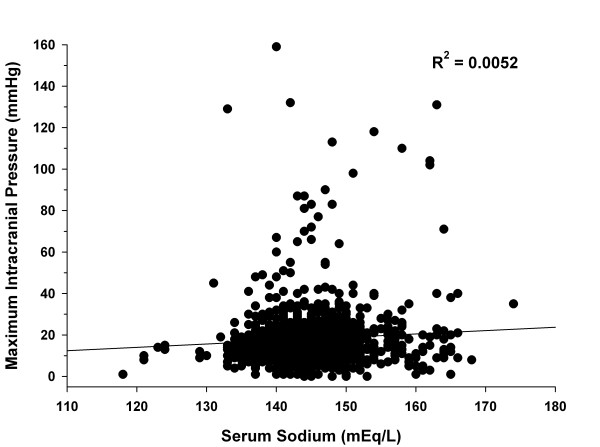
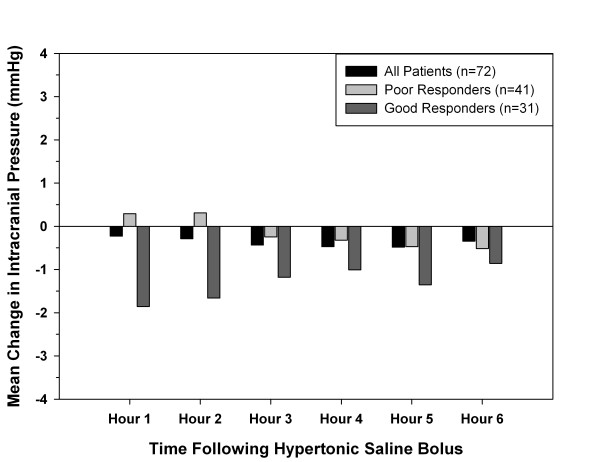
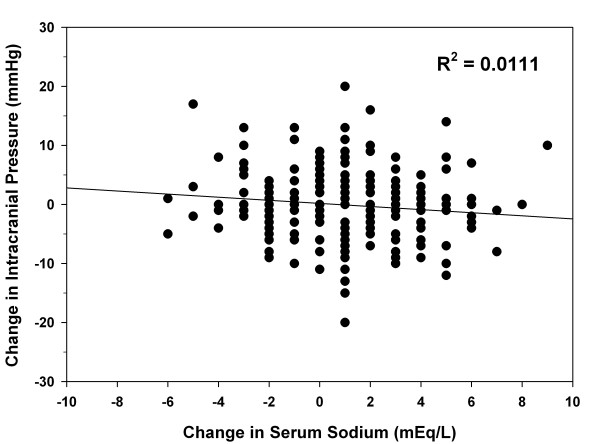
Eighty-one patients were enrolled with mean ± standard deviation age of 36 ± 15 years and median Glasgow Coma Scale score of 7 (interquartile range, 4 to 7). A total of 1,230 serum sodium values (range, 118 to 174 mEq/l) and 7,483 ICP values (range, 0 to 159 mmHg) were collected. There was no correlation between serum sodium and maximum ICP (R(2) = 0.0052). The overall mean ± standard deviation number of interventions for elevated ICP per day was 4.2 ± 2.9, 2.9 ± 2.0, and 2.6 ± 2.3 for patients with a mean serum sodium of < 145, 145 to 155, and > 155 mEq/l, respectively (P < 0.001). Regarding the acute effect of HTS on ICP, there was no statistical difference in mean ICP compared with baseline during hours 1 through 6 following HTS doses (baseline, 13.7 ± 8.4 mmHg; hour 1, 13.6 ± 8.3 mmHg; hour 2, 13.5 ± 8.8 mmHg; hour 3, 13.3 ± 8.7 mmHg; hour 4, 13.4 ± 8.7 mmHg; hour 5, 13.4 ± 8.3 mmHg; hour 6, 13.5 ± 8.3 mmHg; P = 0.84).
Serum sodium concentrations did not correlate with ICP values. These results warrant further evaluation and possible reassessment of sodium goals for ICP management in patients with TBI.
有限的数据表明,轻度高钠血症可能与创伤性脑损伤(TBI)患者的颅内压(ICP)降低有关。研究中心的做法是在TBI患者中使用高渗盐水(HTS)使血清钠目标值达到145至155 mEq/l。本研究的目的是确定血清钠值与ICP之间的关系,并评估HTS对ICP的急性影响。
对2006年1月至2011年3月期间因TBI入住创伤重症监护病房、放置了ICP监测器并接受至少一剂HTS的患者进行回顾性研究。在放置ICP监测器后最多120小时收集数据。主要结局是血清钠与最高ICP之间的关系。次要结局是血清钠与每日控制ICP的平均干预次数之间的关系,以及每次给药后6小时内HTS对ICP的急性影响。采用线性回归分析主要结局。分别采用秩和方差分析及重复测量方差分析来评估干预次数和HTS对ICP的急性影响。
纳入81例患者,平均年龄±标准差为36±15岁,格拉斯哥昏迷量表中位数评分为7(四分位间距,4至7)。共收集到1230个血清钠值(范围为118至174 mEq/l)和7483个ICP值(范围为0至159 mmHg)。血清钠与最高ICP之间无相关性(R² = 0.0052)。血清钠平均<145、145至155、>155 mEq/l的患者,每天因ICP升高进行干预的总体平均±标准差次数分别为4.2±2.9、2.9±2.0和2.6±2.3(P<0.001)。关于HTS对ICP的急性影响,在HTS给药后的1至6小时内,与基线相比,平均ICP无统计学差异(基线,13.7±8.4 mmHg;第1小时,13.6±8.3 mmHg;第2小时,13.5±8.8 mmHg;第3小时,13.3±8.7 mmHg;第4小时,13.4±8.7 mmHg;第5小时,13.4±8.3 mmHg;第6小时,13.5±8.3 mmHg;P = 0.84)。
血清钠浓度与ICP值无相关性。这些结果值得进一步评估,并可能重新评估TBI患者ICP管理的钠目标。