Department of Medicine, Division of Endocrinology, Diabetes and Metabolism, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA 19104, USA.
Endocr Pract. 2013 Jan-Feb;19(1):51-8. doi: 10.4158/EP12115.OR.
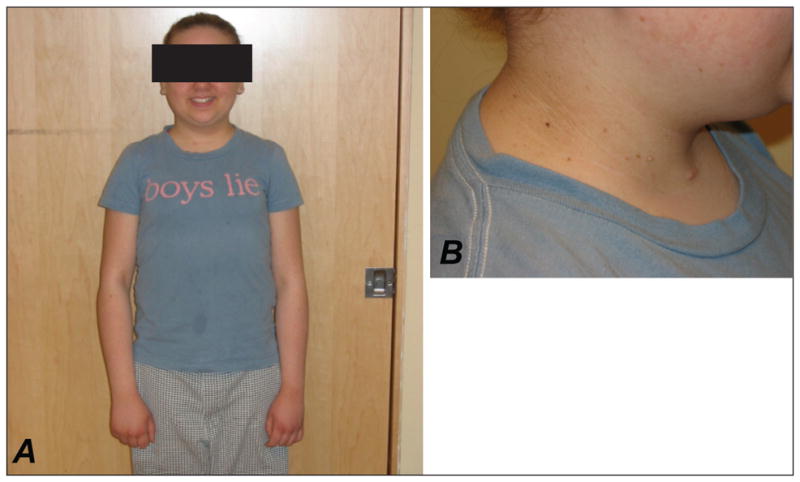
To characterize the metabolic phenotype of 2 cases of normal weight young women who developed type 2 diabetes (T2D), severe insulin resistance (insulin requirement >200 units/day), marked hypertriglyceridemia (>2000 mg/dL), and hepatic steatosis beginning 9 years after undergoing total body irradiation (TBI) and bone marrow transplantation for childhood cancer.
Fasting plasma glucose, insulin, free fatty acids (FFAs), leptin, adiponectin, resistin, TNFα, and IL-6 were measured in each case and in 8 healthy women; Case 1 was also assessed after initiating pioglitazone. Coding regions and splice junctions of PPARG, LMNA, and AKT2 were sequenced in Case 1 and of PPARG in Case 2 to evaluate for familial partial lipodystrophies. Genotyping of APOE was performed in Case 1 to rule out type III hyperlipoproteinemia.
Both cases had elevated plasma levels of insulin, leptin, resistin, and IL-6, high-normal to elevated TNFα, and low to low-normal adiponectin in keeping with post-receptor insulin resistance and adipose tissue inflammation. Case 1 experienced a biochemical response to pioglitazone. No causative mutations for partial lipodystrophies or type III hyperlipoproteinemia were identified.
Though metabolic derangements have previously been reported in association with TBI, few cases have described insulin resistance and hypertriglyceridemia as severe as that seen in our patients. We speculate that early childhood TBI may impede adipose tissue development leading to metabolic complications from an attenuated ability of adipose tissue to accommodate caloric excess, and propose that this extreme metabolic syndrome be evaluated for as a late complication of TBI.
描述 2 例年轻女性的代谢表型,她们在儿童癌症接受全身放疗(TBI)和骨髓移植后 9 年,体重正常但发展为 2 型糖尿病(T2D)、严重胰岛素抵抗(胰岛素需求>200 单位/天)、显著高甘油三酯血症(>2000mg/dL)和肝脂肪变性。
在每例患者和 8 例健康女性中测量空腹血糖、胰岛素、游离脂肪酸(FFAs)、瘦素、脂联素、抵抗素、TNFα 和 IL-6;在开始使用吡格列酮后还对病例 1 进行了评估。在病例 1 中测序了 PPARG、LMNA 和 AKT2 的编码区和剪接接头,并在病例 2 中测序了 PPARG,以评估家族性部分脂肪营养不良。在病例 1 中进行了 APOE 基因分型,以排除 III 型高脂蛋白血症。
两例患者的血浆胰岛素、瘦素、抵抗素和 IL-6 水平升高,TNFα 处于高正常至升高水平,脂联素水平低至正常低值,提示存在受体后胰岛素抵抗和脂肪组织炎症。病例 1 对吡格列酮有生化反应。未发现部分脂肪营养不良或 III 型高脂蛋白血症的致病突变。
尽管之前有报道 TBI 与代谢紊乱有关,但很少有病例描述的胰岛素抵抗和高甘油三酯血症像我们患者那样严重。我们推测,儿童早期 TBI 可能会阻碍脂肪组织的发育,导致代谢并发症,原因是脂肪组织适应热量过剩的能力减弱,我们提出将这种极端的代谢综合征评估为 TBI 的晚期并发症。