Department of Epidemiology, Erasmus MC Rotterdam, dr Molewaterplein 50, Rotterdam, 3015 GE, the Netherlands.
BMC Med. 2012 Dec 6;10:158. doi: 10.1186/1741-7015-10-158.
We developed a Monte Carlo Markov model designed to investigate the effects of modifying cardiovascular disease (CVD) risk factors on the burden of CVD. Internal, predictive, and external validity of the model have not yet been established.
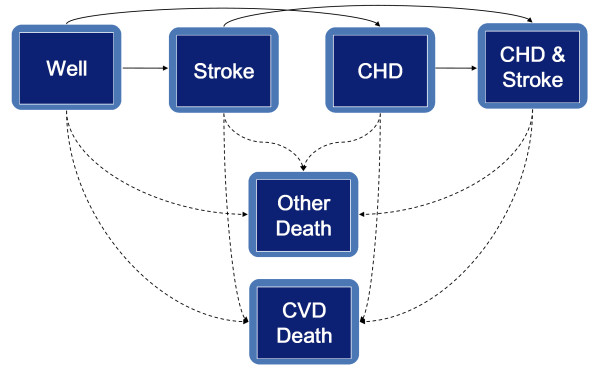
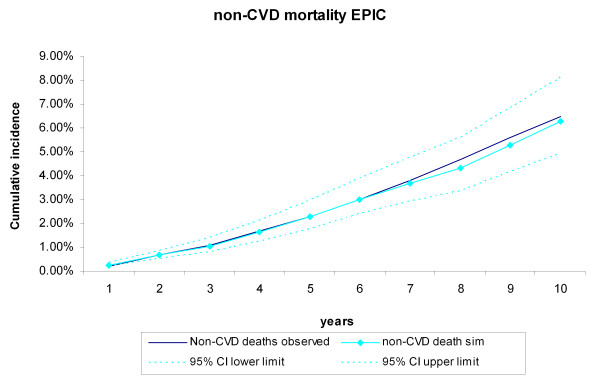
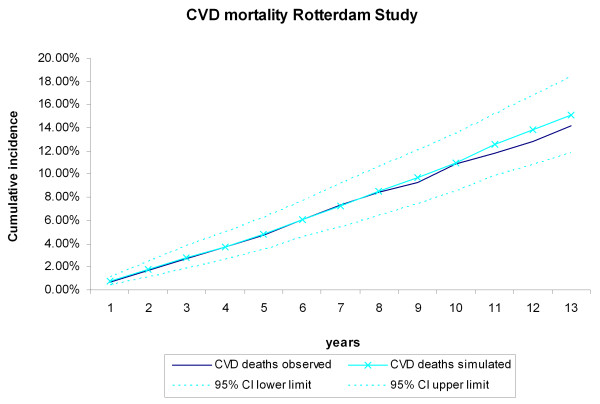
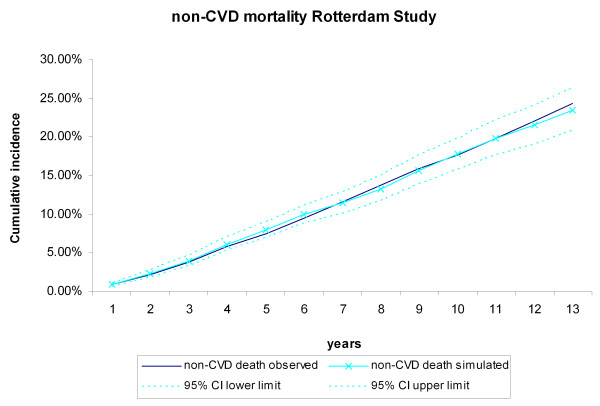
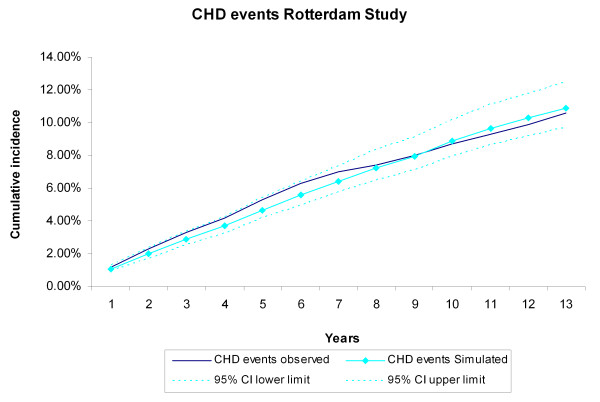
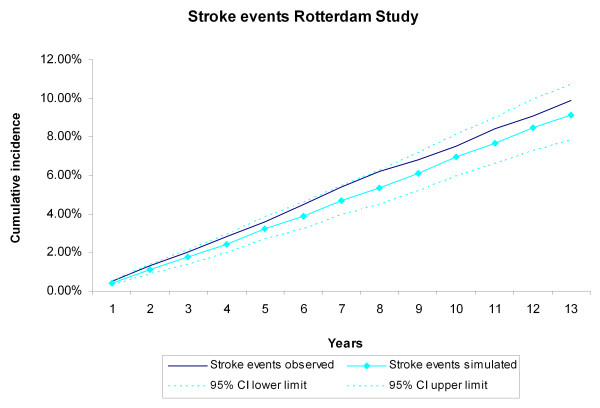
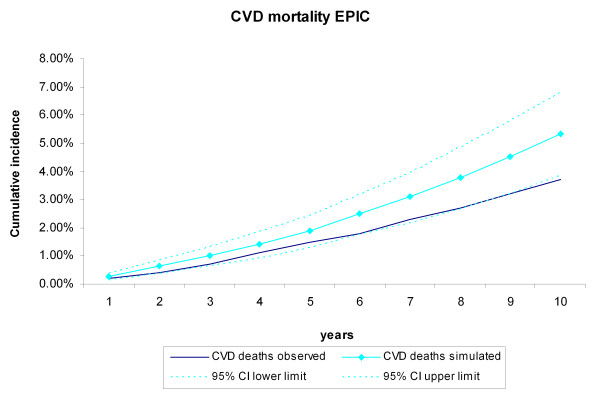
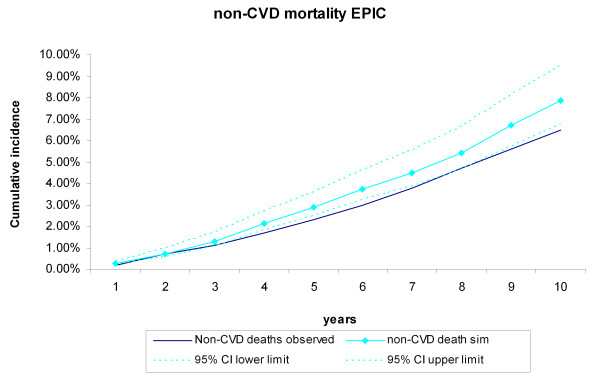
The Rotterdam Ischemic Heart Disease and Stroke Computer Simulation (RISC) model was developed using data covering 5 years of follow-up from the Rotterdam Study. To prove 1) internal and 2) predictive validity, the incidences of coronary heart disease (CHD), stroke, CVD death, and non-CVD death simulated by the model over a 13-year period were compared with those recorded for 3,478 participants in the Rotterdam Study with at least 13 years of follow-up. 3) External validity was verified using 10 years of follow-up data from the European Prospective Investigation of Cancer (EPIC)-Norfolk study of 25,492 participants, for whom CVD and non-CVD mortality was compared.
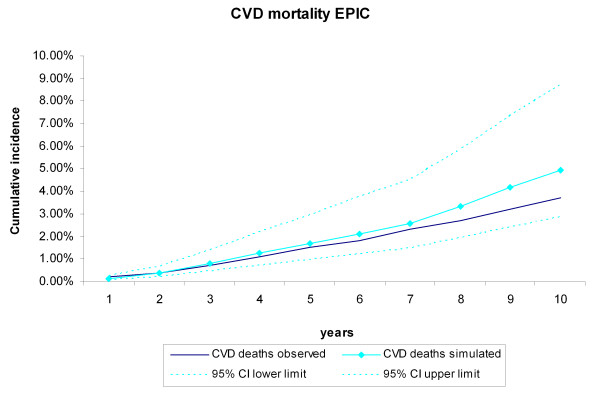
At year 5, the observed incidences (with simulated incidences in brackets) of CHD, stroke, and CVD and non-CVD mortality for the 3,478 Rotterdam Study participants were 5.30% (4.68%), 3.60% (3.23%), 4.70% (4.80%), and 7.50% (7.96%), respectively. At year 13, these percentages were 10.60% (10.91%), 9.90% (9.13%), 14.20% (15.12%), and 24.30% (23.42%). After recalibrating the model for the EPIC-Norfolk population, the 10-year observed (simulated) incidences of CVD and non-CVD mortality were 3.70% (4.95%) and 6.50% (6.29%). All observed incidences fell well within the 95% credibility intervals of the simulated incidences.
We have confirmed the internal, predictive, and external validity of the RISC model. These findings provide a basis for analyzing the effects of modifying cardiovascular disease risk factors on the burden of CVD with the RISC model.
我们开发了一个蒙特卡罗马尔可夫模型,旨在研究改变心血管疾病(CVD)风险因素对 CVD 负担的影响。该模型的内部、预测和外部有效性尚未得到证实。
使用来自鹿特丹研究的 5 年随访数据开发了鹿特丹缺血性心脏病和中风计算机模拟(RISC)模型。为了证明 1)内部和 2)预测的有效性,将模型在 13 年内模拟的冠心病(CHD)、中风、CVD 死亡和非 CVD 死亡的发生率与鹿特丹研究中至少随访 13 年的 3478 名参与者的记录进行了比较。3)使用欧洲前瞻性癌症调查(EPIC)-诺福克研究的 25492 名参与者的 10 年随访数据验证了外部有效性,比较了这些参与者的 CVD 和非 CVD 死亡率。
在第 5 年,3478 名鹿特丹研究参与者的 CHD、中风和 CVD 和非 CVD 死亡率的观察发生率(括号内为模拟发生率)分别为 5.30%(4.68%)、3.60%(3.23%)、4.70%(4.80%)和 7.50%(7.96%)。在第 13 年,这些百分比分别为 10.60%(10.91%)、9.90%(9.13%)、14.20%(15.12%)和 24.30%(23.42%)。对 EPIC-诺福克人群重新校准模型后,CVD 和非 CVD 死亡率的 10 年观察(模拟)发生率分别为 3.70%(4.95%)和 6.50%(6.29%)。所有观察到的发生率都在模拟发生率的 95%可信度区间内。
我们已经证实了 RISC 模型的内部、预测和外部有效性。这些发现为使用 RISC 模型分析改变心血管疾病风险因素对 CVD 负担的影响提供了依据。