Kidney Research Center, Department of Nephrology, Chang Gung Memorial Hospital, Taipei, Taiwan.
PLoS One. 2012;7(12):e51094. doi: 10.1371/journal.pone.0051094. Epub 2012 Dec 7.
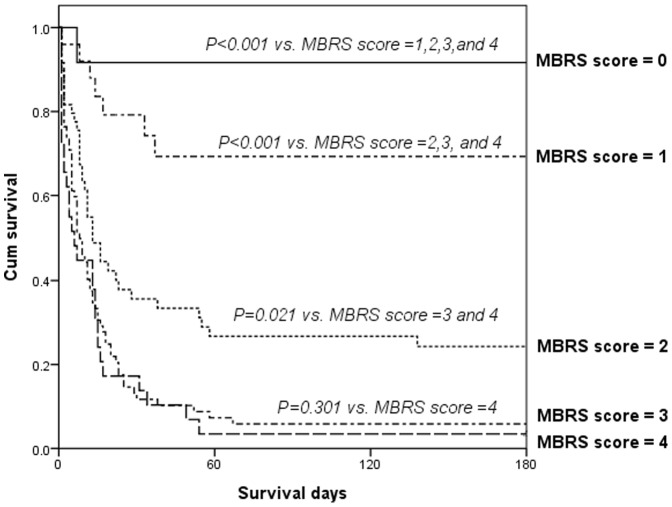
Cirrhotic patients with acute kidney injury (AKI) admitted to intensive care units (ICUs) show extremely high mortality rates. We have proposed the MBRS scoring system, which can be used for assessing patients on the day of admission to the ICU; this new system involves determination of mean arterial pressure (MAP) and bilirubin level and assessment of respiratory failure and sepsis. We had used this scoring system to analyze the prognosis of ICU cirrhotic patients with AKI in 2008, and the current study was an external validation of this scoring system.
A total of 190 cirrhotic patients with AKI were admitted to the ICU between March 2008 and February 2011. We prospectively analyzed and recorded the data for 31 demographic parameters and some clinical characteristic variables on day 1 of admission to the ICU; these variables were considered as predictors of mortality.
The overall in-hospital mortality rate was 73.2% (139/190), and the 6-month mortality rate was 83.2% (158/190). Hepatitis B viral infection (43%) was observed to be the cause of liver disease in most of the patients. Multiple logistic regression analysis indicated that the MBRS and Acute Physiology and Chronic Health Evaluation III (ACPACHE III) scores determined on the first day of admission to the ICU were independent predictors of in-hospital mortality in patients. In the analysis of the area under the receiver operating characteristic (AUROC) curves, the MBRS scores showed good discrimination (AUROC: 0.863±0.032, p<0.001) in predicting in-hospital mortality.
On the basis of the results of this external validation, we conclude that the MBRS scoring system is a reproducible, simple, easy-to-apply evaluation tool that can increase the prediction accuracy of short-term prognosis in critically ill cirrhotic patients with AKI.
入住重症监护病房(ICU)的肝硬化合并急性肾损伤(AKI)患者死亡率极高。我们提出了 MBRS 评分系统,该系统可用于评估 ICU 入院当天的患者;新系统涉及平均动脉压(MAP)和胆红素水平的测定,并评估呼吸衰竭和脓毒症。我们曾在 2008 年使用该评分系统分析 ICU 肝硬化合并 AKI 患者的预后,本研究是对该评分系统的外部验证。
2008 年 3 月至 2011 年 2 月,共有 190 例肝硬化合并 AKI 患者入住 ICU。我们前瞻性分析并记录了患者入住 ICU 第 1 天的 31 个人口统计学参数和一些临床特征变量的数据;这些变量被认为是死亡率的预测因素。
总体院内死亡率为 73.2%(139/190),6 个月死亡率为 83.2%(158/190)。大多数患者的乙型肝炎病毒感染(43%)被认为是肝脏疾病的原因。多因素逻辑回归分析表明,入住 ICU 第 1 天的 MBRS 和急性生理学和慢性健康评估 III(APACHE III)评分是患者院内死亡的独立预测因素。在接受者操作特征(ROC)曲线下面积(AUROC)分析中,MBRS 评分显示出良好的区分度(AUROC:0.863±0.032,p<0.001),可预测院内死亡率。
基于这项外部验证的结果,我们得出结论,MBRS 评分系统是一种可重复、简单、易于应用的评估工具,可以提高危重症肝硬化合并 AKI 患者短期预后的预测准确性。