Department of Intensive Care, University New South Wales Clinical School, The Prince of Wales Hospital, Randwick, NSW, Australia.
Intensive Care Med. 2013 May;39(5):910-8. doi: 10.1007/s00134-013-2830-2. Epub 2013 Jan 24.
To ascertain the relationship among early (first 48 h) deep sedation, time to extubation, delirium and long-term mortality.
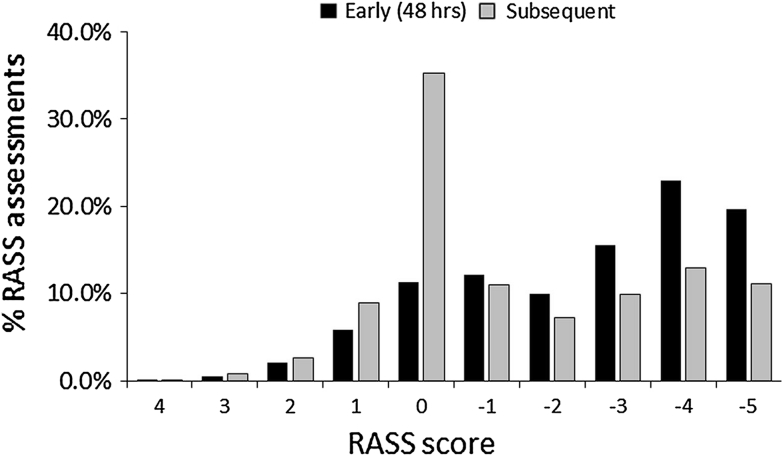
We conducted a multicentre prospective longitudinal cohort study in 11 Malaysian hospitals including medical/surgical patients (n = 259) who were sedated and ventilated ≥24 h. Patients were followed from ICU admission up to 28 days in ICU with 4-hourly sedation and daily delirium assessments and 180-day mortality. Deep sedation was defined as Richmond Agitation Sedation Score (RASS) ≤-3.
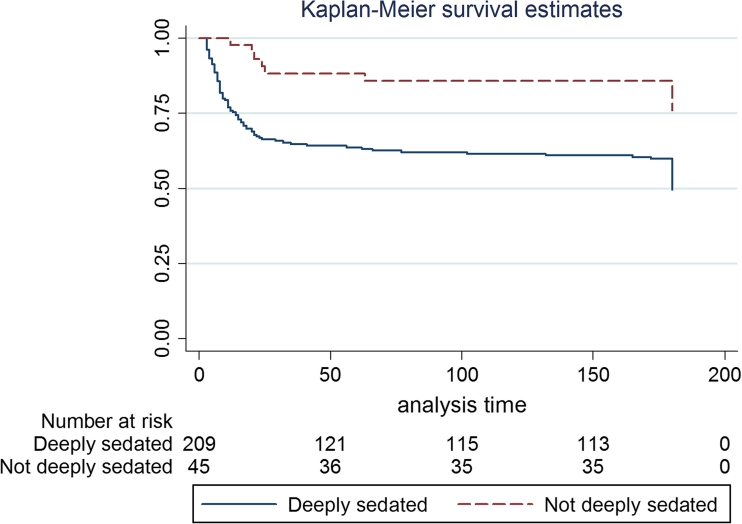
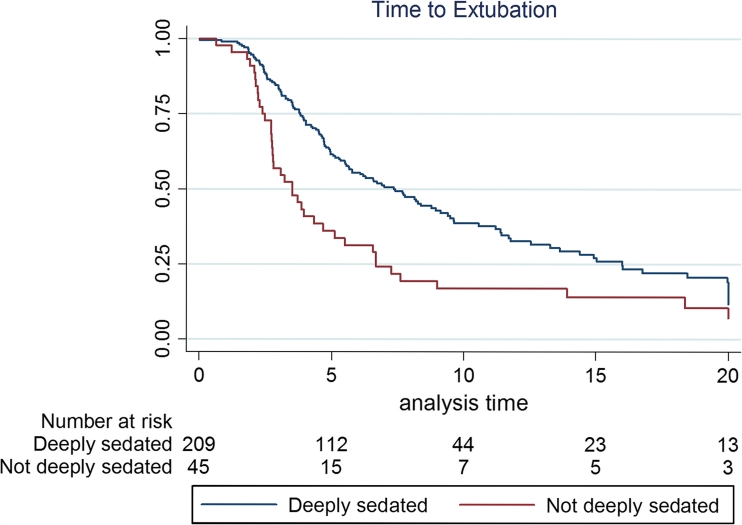
The cohort had a mean (SD) age of 53.1 (15.9) years and APACHE II score of 21.3 (8.2) with hospital and 180-day mortality of 82 (31.7%) and 110/237 (46.4%). Patients were followed for 2,657 ICU days and underwent 13,836 RASS assessments. Midazolam prescription was predominant compared to propofol, given to 241 (93%) versus 72 (28%) patients (P < 0.0001) for 966 (39.6%) versus 183 (7.5%) study days respectively. Deep sedation occurred in (182/257) 71% patients at first assessment and in 159 (61%) patients and 1,658 (59%) of all RASS assessments at 48 h. Multivariable Cox proportional hazard regression analysis adjusting for a priori assigned covariates including sedative agents, diagnosis, age, APACHE II score, operative, elective, vasopressors and dialysis showed that early deep sedation was independently associated with longer time to extubation [hazard ratio (HR) 0.93, 95% confidence interval (CI) 0.89-0.97, P = 0.003], hospital death (HR 1.11, 95% CI 1.05-1.18, P < 0.001) and 180-day mortality (HR 1.09, 95% CI 1.04-1.15, P = 0.002), but not time to delirium (HR 0.98, P = 0.23). Delirium occurred in 114 (44%) of patients.
Irrespective of sedative choice, early deep sedation was independently associated with delayed extubation and higher mortality, and thus was a potentially modifiable risk in interventional trials.
确定早期(48 小时内)深度镇静、拔管时间、谵妄与长期死亡率之间的关系。
我们在马来西亚的 11 家医院进行了一项多中心前瞻性纵向队列研究,纳入了接受镇静和通气治疗≥24 小时的内科/外科患者(n=259)。从 ICU 入院开始,患者接受 28 天的 ICU 随访,每 4 小时进行一次镇静评估,每天进行一次谵妄评估,并在 180 天进行死亡率评估。深度镇静定义为 Richmond 躁动镇静评分(RASS)≤-3。
该队列的平均(标准差)年龄为 53.1(15.9)岁,APACHE II 评分为 21.3(8.2)分,院内死亡率和 180 天死亡率分别为 82(31.7%)和 110/237(46.4%)。患者接受了 2657 天 ICU 治疗,进行了 13836 次 RASS 评估。咪达唑仑的处方量明显多于丙泊酚,241 例(93%)患者使用咪达唑仑,72 例(28%)患者使用丙泊酚(P<0.0001),咪达唑仑分别用于 966 天(39.6%)和 183 天(7.5%)的研究。首次评估时,71%(182/257)的患者出现深度镇静,在 48 小时时,159 例(61%)患者和 1658 次(59%)RASS 评估中出现深度镇静。多变量 Cox 比例风险回归分析调整了预先指定的协变量,包括镇静剂、诊断、年龄、APACHE II 评分、手术、急诊、血管加压素和透析,结果表明,早期深度镇静与更长的拔管时间[风险比(HR)0.93,95%置信区间(CI)0.89-0.97,P=0.003]、院内死亡(HR 1.11,95% CI 1.05-1.18,P<0.001)和 180 天死亡率(HR 1.09,95% CI 1.04-1.15,P=0.002)独立相关,但与谵妄时间无关(HR 0.98,P=0.23)。114 例(44%)患者发生了谵妄。
无论镇静药物的选择如何,早期深度镇静与拔管时间延迟和死亡率升高独立相关,因此在干预性试验中是一个潜在可改变的风险因素。