Liverpool School of Tropical Medicine, Liverpool, United Kingdom.
JAMA. 2013 Feb 13;309(6):594-604. doi: 10.1001/jama.2012.216231.
Intermittent preventive therapy with sulfadoxine-pyrimethamine to control malaria during pregnancy is used in 37 countries in sub-Saharan Africa, and 31 of those countries use the standard 2-dose regimen. However, 2 doses may not provide protection during the last 4 to 10 weeks of pregnancy, a pivotal period for fetal weight gain.
To perform a systematic review and meta-analysis of trials to determine whether regimens containing 3 or more doses of sulfadoxine-pyrimethamine for intermittent preventive therapy during pregnancy are associated with a higher birth weight or lower risk of low birth weight (LBW) (<2500 g) than standard 2-dose regimens.
ISI Web of Knowledge, EMBASE, SCOPUS, PubMed, LILACS, the Malaria in Pregnancy Library, Cochrane CENTRAL, and trial registries from their inception to December 2012, without language restriction. Eligible studies included randomized and quasi-randomized trials of intermittent preventive therapy during pregnancy with sulfadoxine-pyrimethamine monotherapy.
Data were independently abstracted by 2 investigators. Relative risk (RR), mean differences, and 95% CIs were calculated with random-effects models.
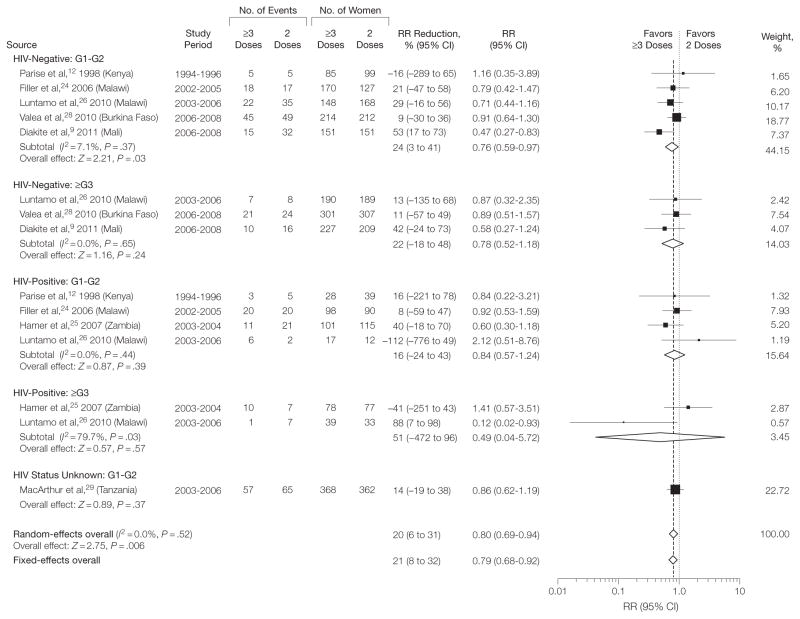
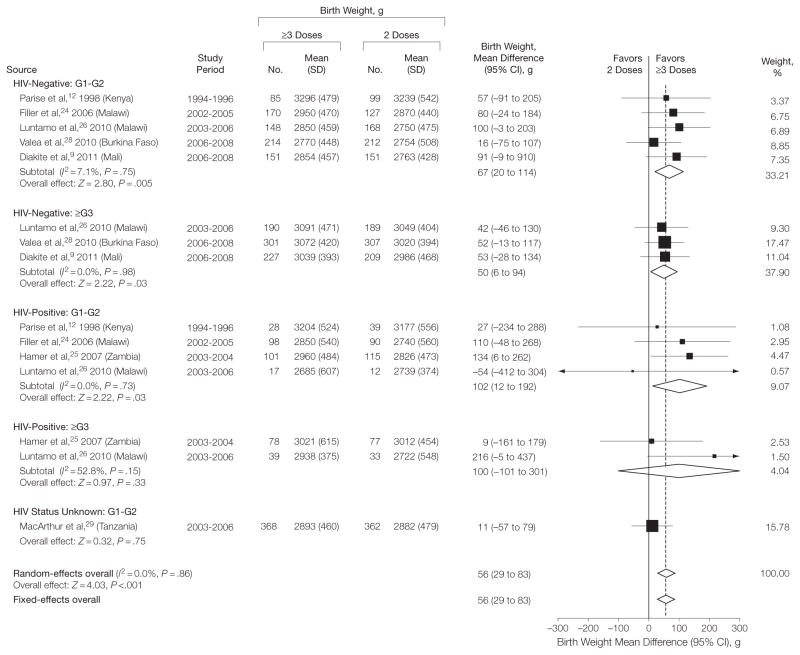
Of 241 screened studies, 7 trials of 6281 pregnancies were included. The median birth weight in the 2-dose group was 2870 g (range, 2722-3239 g) and on average 56 g higher (95% CI, 29-83 g; I2 = 0%) in the ≥3-dose group. Three or more doses were associated with fewer LBW births (RR, 0.80; 95% CI, 0.69-0.94; I 2 = 0%), with a median LBW risk per 1000 women in the 2-dose group (assumed control group risk) of 167 per 1000 vs 134 per 1000 in the ≥3-dose group (absolute risk reduction, 33 per 1000 [95% CI, 10-52]; number needed to treat = 31). The association was consistent across a wide range of sulfadoxine-pyrimethamine resistance (0% to 96% dihydropteroate-synthase K540E mutations). There was no evidence of small-study bias. The ≥3-dose group had less placental malaria (RR, 0.51; 95% CI, 0.38-0.68; I 2 = 0%, in 6 trials, 63 vs 32 per 1000; absolute risk reduction, 31 per 1000 [95% CI, 20-39]). In primigravid plus secundigravid women, the risk of moderate to severe maternal anemia was lower in the ≥3-dose group (RR, 0.60; 95% CI, 0.36-0.99; I2 = 20%; in 6 trials, 36 vs 22 per 1000; absolute risk reduction, 14 per 1000 [95% CI, 0.4-23]). There were no differences in rates of serious adverse events.
Among pregnant women in sub-Saharan Africa, intermittent preventive therapy with 3 or more doses of sulfadoxine-pyrimethamine was associated with a higher birth weight and lower risk of LBW than the standard 2-dose regimens. These data provide support for the new WHO recommendations to provide at least 3 doses of intermittent preventive therapy during pregnancy at each scheduled antenatal care visit in the second and third trimester.
在撒哈拉以南非洲的 37 个国家,使用磺胺多辛-乙胺嘧啶间歇性预防疗法来控制怀孕期间的疟疾,其中 31 个国家使用标准的 2 剂方案。然而,在妊娠的最后 4 到 10 周,这是胎儿体重增加的关键时期,两剂可能无法提供保护。
进行系统回顾和荟萃分析,以确定在怀孕期间使用磺胺多辛-乙胺嘧啶进行间歇性预防治疗的方案中包含 3 剂或更多剂量是否与更高的出生体重或更低的低出生体重(LBW)(<2500 克)风险相关,而不是标准的 2 剂方案。
ISI Web of Knowledge、EMBASE、SCOPUS、PubMed、LILACS、妊娠疟疾文库、Cochrane 中央和试验注册处,从成立到 2012 年 12 月,无语言限制。合格的研究包括随机和半随机试验,在怀孕期间使用磺胺多辛-乙胺嘧啶单药治疗间歇性预防疗法。
两名研究人员独立提取数据。相对风险(RR)、均值差异和 95%置信区间采用随机效应模型计算。
在筛选出的 241 项研究中,有 7 项关于 6281 例妊娠的试验被纳入。在 2 剂组中,平均出生体重为 2870 克(范围为 2722-3239 克),而在 ≥3 剂组中,平均出生体重高 56 克(95%置信区间,29-83 克;I2 = 0%)。三剂或更多剂量与较低的 LBW 出生(RR,0.80;95%置信区间,0.69-0.94;I2 = 0%)相关,在 2 剂组中,每 1000 名妇女中 LBW 的风险为每 1000 名妇女中 167 名(假设对照组风险),而在 ≥3 剂组中,每 1000 名妇女中 134 名(绝对风险降低,33 名/1000 [95%置信区间,10-52];需要治疗的人数= 31)。这种关联在广泛的磺胺多辛-乙胺嘧啶耐药范围内是一致的(0%至 96%二氢叶酸合成酶 K540E 突变)。没有证据表明存在小研究偏倚。在≥3 剂组中,胎盘疟疾较少(RR,0.51;95%置信区间,0.38-0.68;I2 = 0%,在 6 项试验中,每 1000 名中有 63 名 vs 32 名;绝对风险降低,31 名/1000 [95%置信区间,20-39])。在初产妇和经产妇中,≥3 剂组中度至重度孕妇贫血的风险较低(RR,0.60;95%置信区间,0.36-0.99;I2 = 20%;在 6 项试验中,每 1000 名中有 36 名 vs 22 名;绝对风险降低,14 名/1000 [95%置信区间,0.4-23])。两组严重不良事件发生率无差异。
在撒哈拉以南非洲的孕妇中,磺胺多辛-乙胺嘧啶间歇性预防治疗 3 剂或更多剂量与标准的 2 剂方案相比,出生体重较高,LBW 风险较低。这些数据支持世卫组织的新建议,即在妊娠的第二和第三个三个月的每次定期产前保健就诊时,提供至少 3 剂间歇性预防治疗。