Department of Public Health and Primary Care, Leiden University Medical Centre, Postzone V-0-P, PO Box 9600, 2300, Leiden, RC, The Netherlands.
BMC Fam Pract. 2013 Feb 26;14:29. doi: 10.1186/1471-2296-14-29.
Until now, cardiometabolic risk assessment in Dutch primary health care was directed at case-finding, and structured, programmatic prevention is lacking. Therefore, the Prevention Consultation cardiometabolic risk (PC CMR), a stepwise approach to identify and manage patients with cardiometabolic risk factors, was developed. The aim of this study was 1) to evaluate uptake rates of the two steps of the PC CMR, 2) to assess the rates of newly diagnosed hypertension, hypercholesterolemia, diabetes mellitus and chronic kidney disease and 3) to explore reasons for non-participation.
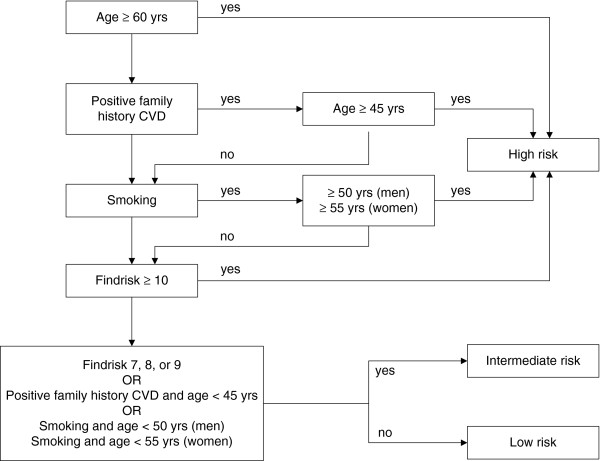
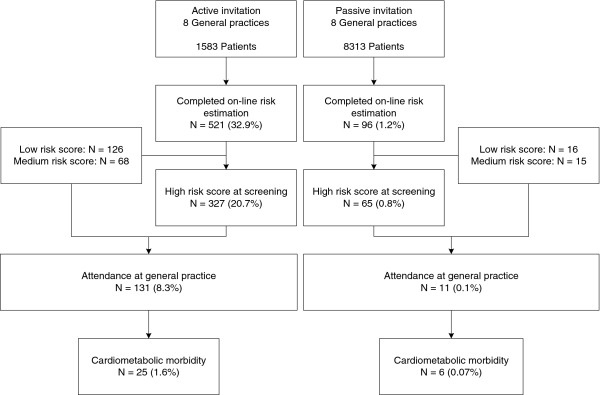
Sixteen general practices throughout the Netherlands were recruited to implement the PC CMR during 6 months. In eight practices eligible patients aged between 45 and 70 years without a cardiometabolic disease were actively invited by a personal letter ('active approach') and in eight other practices eligible patients were informed about the PC CMR only by posters and leaflets in the practice ('passive approach'). Participating patients completed an online risk estimation (first step). Patients estimated as having a high risk according to the online risk estimation were advised to visit their general practice to complete the risk profile with blood pressure measurements and blood tests for cholesterol and glucose and to receive recommendations about risk lowering interventions (second step).
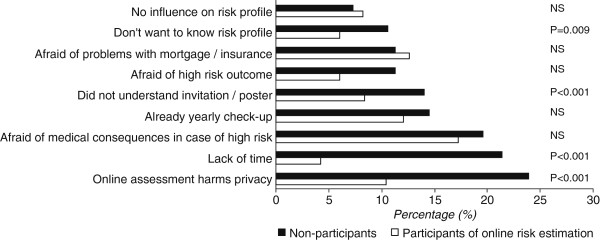
The online risk estimation was completed by 521 (33%) and 96 (1%) of patients in the practices with an active and passive approach, respectively. Of these patients 392 (64%) were estimated to have a high risk and were referred to the practice; 142 of 392 (36%) consulted the GP. A total of 31 (22%) newly diagnosed patients were identified. Hypertension, hypercholesterolemia, diabetes and chronic kidney disease were diagnosed in 13%, 11%, 1% and 0%, respectively. Privacy risks were the most frequently mentioned reason not to participate.
One third of the patients responded to an active invitation to complete an online risk estimation. A passive invitation resulted in only a small number of participating patients. Two third of the participants of the online risk estimation had a high risk, but only one third of them attended the GP office. One in five visiting patients had a diagnosed cardiometabolic risk factor or disease.
到目前为止,荷兰初级保健中心的心脏代谢风险评估一直针对病例发现,缺乏结构化、计划性的预防措施。因此,开发了预防咨询心脏代谢风险(PC CMR),这是一种逐步识别和管理心脏代谢风险因素患者的方法。本研究的目的是 1)评估 PC CMR 的两个步骤的参与率,2)评估新诊断的高血压、高胆固醇血症、糖尿病和慢性肾脏病的发生率,3)探讨不参与的原因。
荷兰的 16 家全科诊所被招募来在 6 个月内实施 PC CMR。在 8 家诊所中,通过个人信件主动邀请年龄在 45 至 70 岁之间且无心脏代谢疾病的符合条件的患者(“主动方法”),而在另外 8 家诊所中,仅通过诊所中的海报和传单向符合条件的患者告知 PC CMR(“被动方法”)。参与的患者完成在线风险评估(第一步)。根据在线风险评估,估计风险较高的患者被建议前往他们的全科医生诊所完成风险概况,包括血压测量和胆固醇和葡萄糖血液检查,并收到关于降低风险干预措施的建议(第二步)。
在采用主动和被动方法的诊所中,分别有 521 名(33%)和 96 名(1%)患者完成了在线风险评估。这些患者中有 392 名(64%)被估计有高风险,并被转介到诊所;其中 392 名中有 142 名(36%)咨询了全科医生。共发现 31 名(22%)新诊断的患者。诊断出高血压、高胆固醇血症、糖尿病和慢性肾脏病的患者分别占 13%、11%、1%和 0%。隐私风险是不参与的最常提到的原因。
三分之一的患者对完成在线风险评估的主动邀请做出了回应。被动邀请仅导致少数参与患者。在线风险评估的参与者中有三分之二的人风险较高,但其中只有三分之一的人去看了全科医生。在就诊的患者中,五分之一的人患有已诊断的心脏代谢风险因素或疾病。