Krinsley James S, Egi Moritoki, Kiss Alex, Devendra Amin N, Schuetz Philipp, Maurer Paula M, Schultz Marcus J, van Hooijdonk Roosmarijn T M, Kiyoshi Morita, Mackenzie Iain M J, Annane Djillali, Stow Peter, Nasraway Stanley A, Holewinski Sharon, Holzinger Ulrike, Preiser Jean-Charles, Vincent Jean-Louis, Bellomo Rinaldo
Crit Care. 2013 Mar 1;17(2):R37. doi: 10.1186/cc12547.
Hyperglycemia, hypoglycemia, and increased glycemic variability have each been independently associated with increased risk of mortality in critically ill patients. The role of diabetic status on modulating the relation of these three domains of glycemic control with mortality remains uncertain. The purpose of this investigation was to determine how diabetic status affects the relation of hyperglycemia, hypoglycemia, and increased glycemic variability with the risk of mortality in critically ill patients.
This is a retrospective analysis of prospectively collected data involving 44,964 patients admitted to 23 intensive care units (ICUs) from nine countries, between February 2001 and May 2012. We analyzed mean blood glucose concentration (BG), coefficient of variation (CV), and minimal BG and created multivariable models to analyze their independent association with mortality. Patients were stratified according to the diagnosis of diabetes.
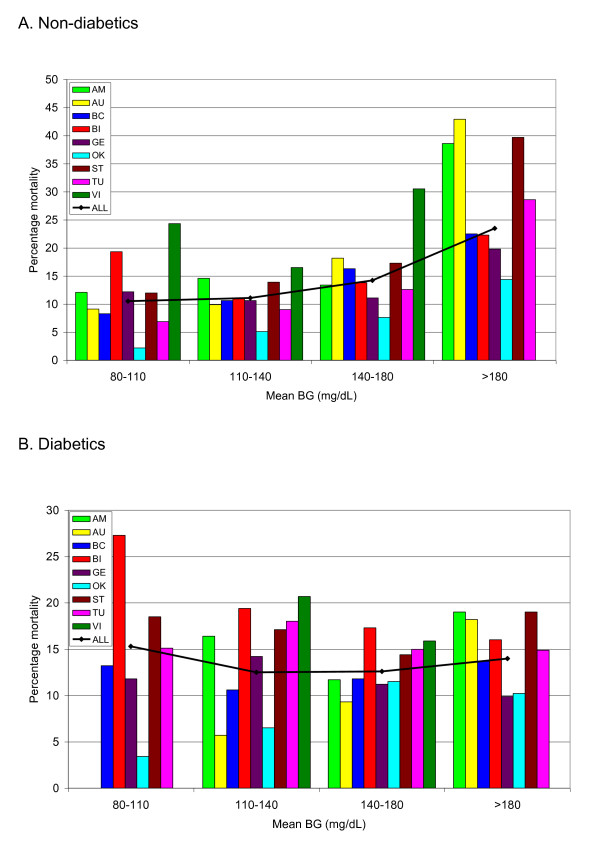
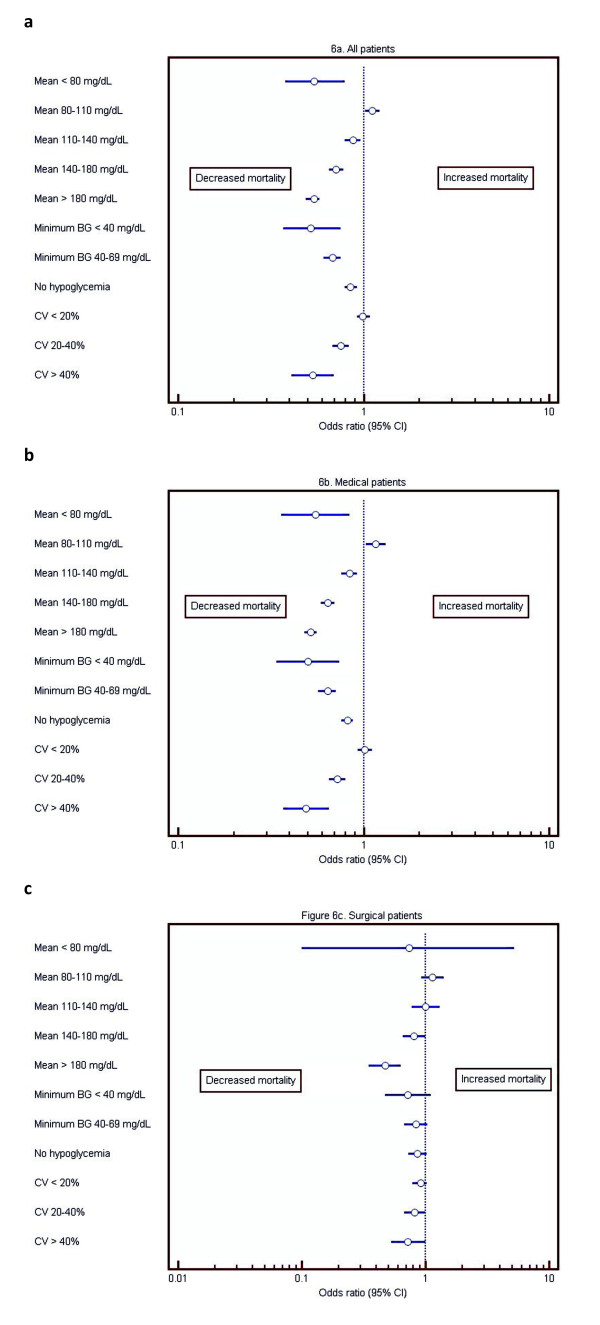
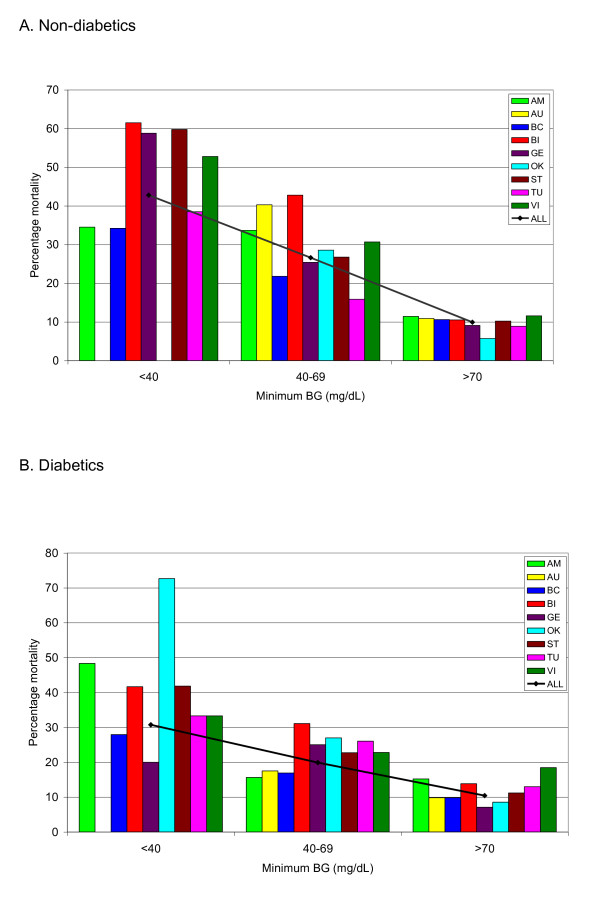
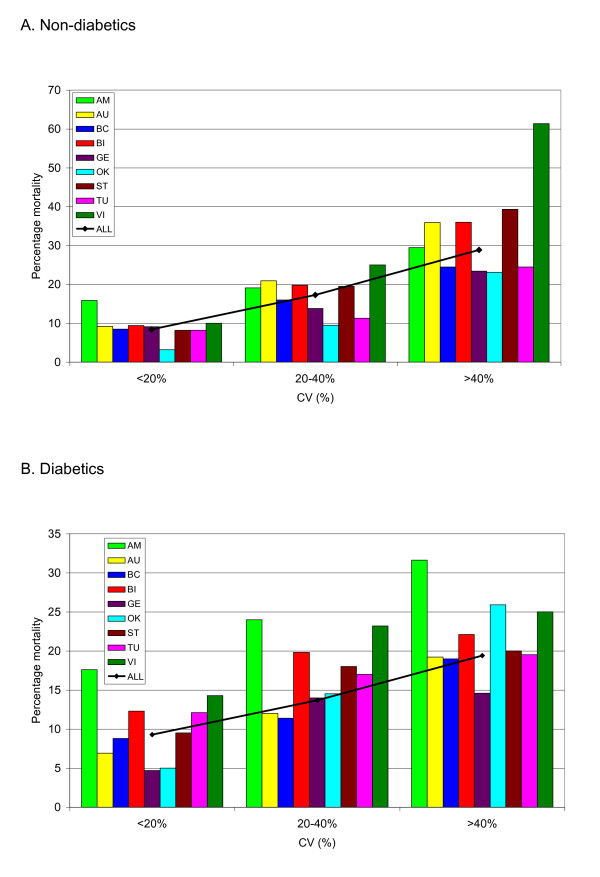
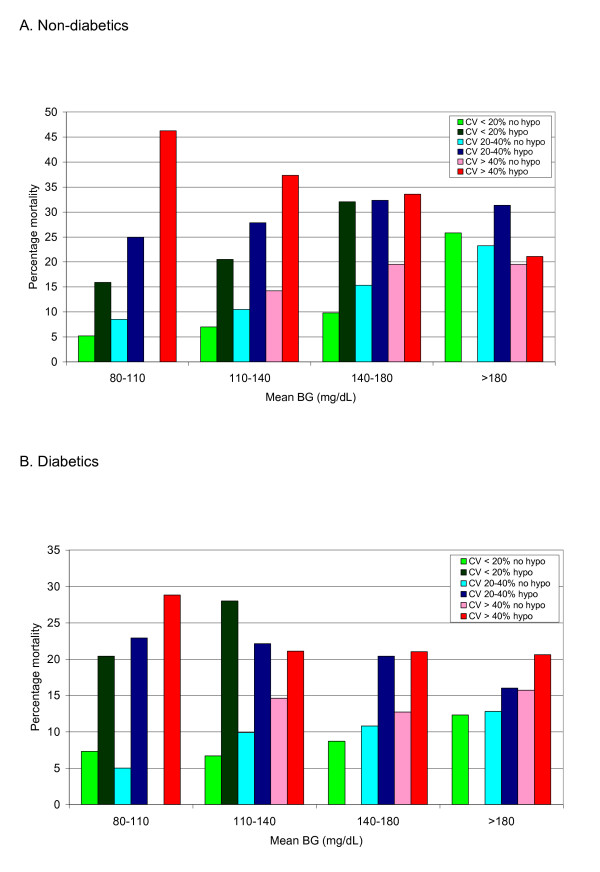
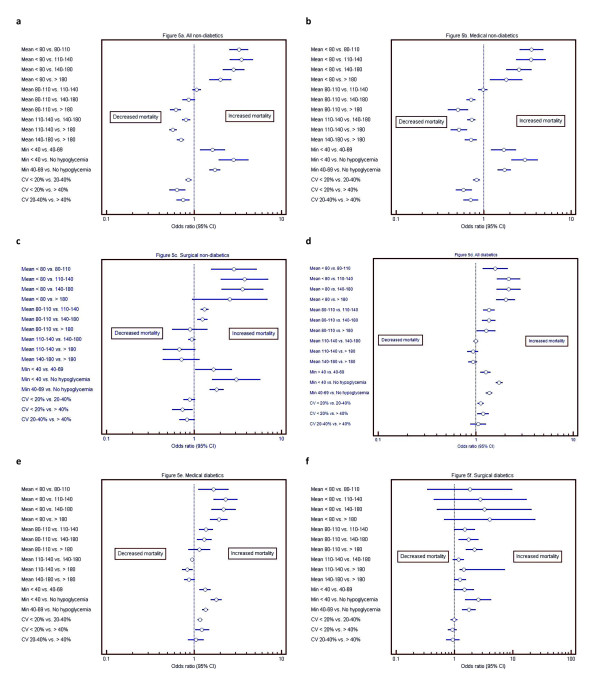
Among patients without diabetes, mean BG bands between 80 and 140 mg/dl were independently associated with decreased risk of mortality, and mean BG bands>or=140 mg/dl, with increased risk of mortality. Among patients with diabetes, mean BG from 80 to 110 mg/dl was associated with increased risk of mortality and mean BG from 110 to 180 mg/dl with decreased risk of mortality. An effect of center was noted on the relation between mean BG and mortality. Hypoglycemia, defined as minimum BG<70 mg/dl, was independently associated with increased risk of mortality among patients with and without diabetes and increased glycemic variability, defined as CV>or=20%, was independently associated with increased risk of mortality only among patients without diabetes. Derangements of more than one domain of glycemic control had a cumulative association with mortality, especially for patients without diabetes.
Although hyperglycemia, hypoglycemia, and increased glycemic variability is each independently associated with mortality in critically ill patients, diabetic status modulates these relations in clinically important ways. Our findings suggest that patients with diabetes may benefit from higher glucose target ranges than will those without diabetes. Additionally, hypoglycemia is independently associated with increased risk of mortality regardless of the patient's diabetic status, and increased glycemic variability is independently associated with increased risk of mortality among patients without diabetes.
高血糖、低血糖以及血糖变异性增加均与危重症患者死亡率升高独立相关。糖尿病状态在调节这三个血糖控制领域与死亡率之间关系中的作用仍不确定。本研究的目的是确定糖尿病状态如何影响高血糖、低血糖以及血糖变异性增加与危重症患者死亡风险之间的关系。
这是一项对前瞻性收集的数据进行的回顾性分析,涉及2001年2月至2012年5月期间来自9个国家的23个重症监护病房(ICU)收治的44964例患者。我们分析了平均血糖浓度(BG)、变异系数(CV)和最低血糖,并建立多变量模型来分析它们与死亡率的独立关联。患者根据糖尿病诊断进行分层。
在无糖尿病患者中,80至140mg/dl的平均血糖范围与死亡风险降低独立相关,而平均血糖范围≥140mg/dl与死亡风险增加相关。在糖尿病患者中,80至110mg/dl的平均血糖与死亡风险增加相关,110至180mg/dl的平均血糖与死亡风险降低相关。观察到中心对平均血糖与死亡率之间的关系有影响。低血糖定义为最低血糖<70mg/dl,在有糖尿病和无糖尿病患者中均与死亡风险增加独立相关,血糖变异性增加定义为CV≥20%,仅在无糖尿病患者中与死亡风险增加独立相关。多个血糖控制领域的紊乱与死亡率有累积关联,尤其是对于无糖尿病患者。
尽管高血糖、低血糖以及血糖变异性增加均与危重症患者死亡率独立相关,但糖尿病状态以临床上重要的方式调节这些关系。我们的研究结果表明,糖尿病患者可能比非糖尿病患者从更高的血糖目标范围中获益。此外,无论患者的糖尿病状态如何,低血糖均与死亡风险增加独立相关,而血糖变异性增加在无糖尿病患者中与死亡风险增加独立相关。