Cardiovascular Nutrition Laboratory, Jean Mayer USDA Human Nutrition Research Center on Aging, Tufts University, Boston, MA 02111, USA.
J Am Heart Assoc. 2013 Feb 19;2(1):e005066. doi: 10.1161/JAHA.112.005066.
Available data are inconsistent regarding factors influencing plasma cholesterol homeostasis marker concentrations and their value in predicting subsequent cardiovascular disease (CVD) events.
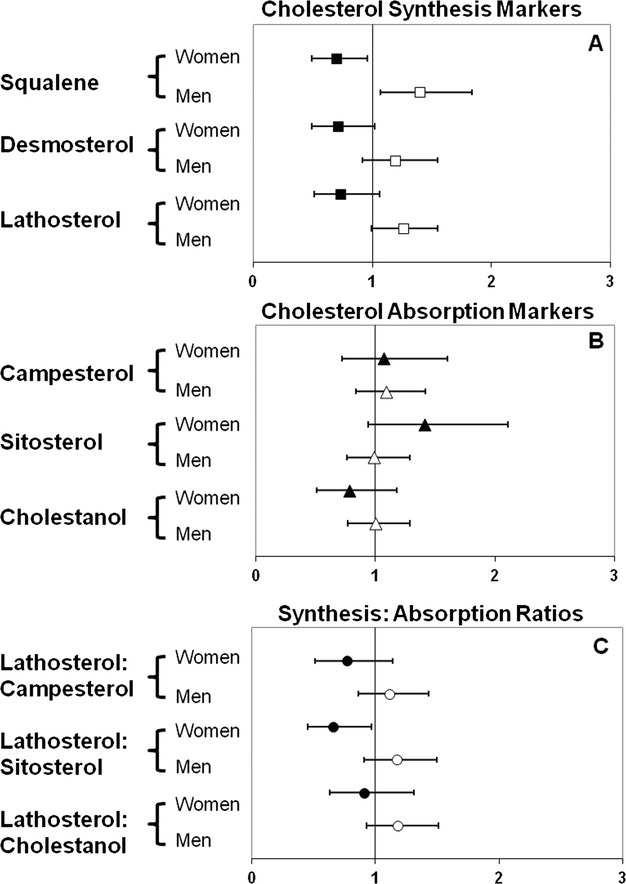
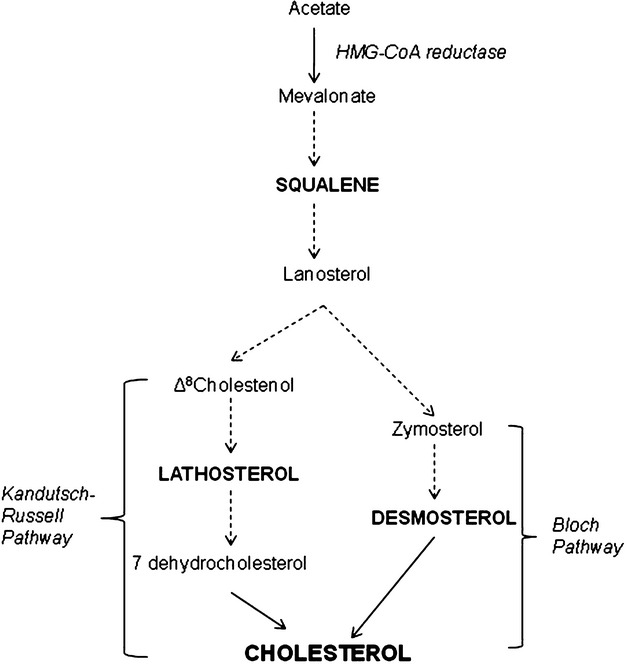
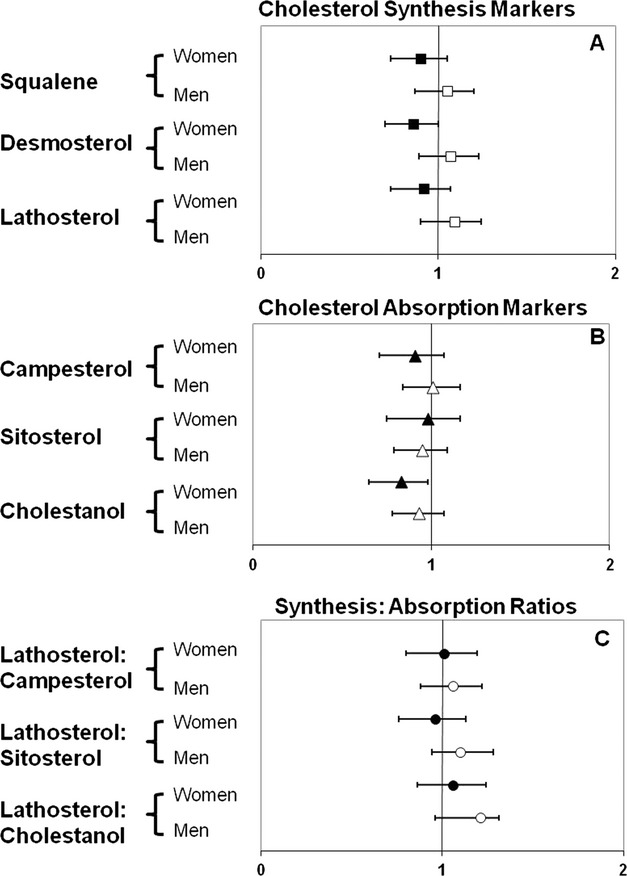
To address this issue, the relationship between markers of cholesterol absorption (campesterol, sitosterol, cholestanol) and synthesis (squalene, desmosterol, lathosterol) and 10-year CVD incidence was assessed in Framingham Offspring Study participants (cycle 6) who were without CVD at baseline and not taking lipid-lowering medications (N=2616). The primary end point was "hard" coronary heart disease (HCHD; coronary death and myocardial infarction), and the secondary end point was full CVD (HCHD plus stroke, coronary insufficiency, angina pectoris, peripheral artery disease, and congestive heart failure). In cross-sectional analysis, significant differences by sex, age, body mass index, blood pressure, and smoking status were observed. In both women and men, lower cholesterol absorption was associated with higher triglyceride and lower high-density lipoprotein (HDL) cholesterol concentrations, whereas lower cholesterol synthesis was associated with higher low-density lipoprotein (LDL) cholesterol concentrations (P for trend <0.05). In women only, lower cholesterol synthesis and absorption were associated with higher non-HDL cholesterol concentrations. Using Cox proportional hazards model adjusting for standard CVD risk factors, squalene concentrations were associated with lower HCHD in women (hazard ratio=0.70 [0.5 to 0.9]). In contrast, squalene (hazard ratio=1.40 [1.1 to 1.8]) concentrations were associated with higher HCHD in men (P<0.0001 for interaction). The cholesterol absorption markers were not predictive of HCHD or full CVD in either women or men.
These data suggest significant sex differences in the 10-year prognostic value of cholesterol synthesis markers and HCHD, specifically coronary death and incidence of myocardial infarction.
URL:http://ClinicalTrials.gov. Unique identifier: NCT00074464.
关于影响血浆胆固醇稳态标志物浓度的因素及其在预测随后发生心血管疾病(CVD)事件中的价值,现有数据并不一致。
为了解决这个问题,我们在Framingham Offspring 研究参与者(第 6 周期)中评估了胆固醇吸收(菜固醇、谷固醇、胆甾烷醇)和合成(角鲨烯、去甲固醇、羊毛固醇)标志物与 10 年 CVD 发生率之间的关系,这些参与者在基线时没有 CVD,并且没有服用降脂药物(N=2616)。主要终点是“硬性”冠心病(HCHD;冠心病死亡和心肌梗死),次要终点是全因 CVD(HCHD 加上卒中、冠状动脉功能不全、心绞痛、外周动脉疾病和充血性心力衰竭)。在横断面分析中,观察到性别、年龄、体重指数、血压和吸烟状况存在显著差异。在女性和男性中,胆固醇吸收降低与甘油三酯升高和高密度脂蛋白(HDL)胆固醇浓度降低有关,而胆固醇合成降低与低密度脂蛋白(LDL)胆固醇浓度升高有关(趋势 P 值<0.05)。仅在女性中,胆固醇合成和吸收降低与非 HDL 胆固醇浓度升高有关。使用 Cox 比例风险模型调整标准 CVD 危险因素后,角鲨烯浓度与女性 HCHD 降低相关(风险比=0.70[0.5 至 0.9])。相比之下,角鲨烯(风险比=1.40[1.1 至 1.8])浓度与男性 HCHD 升高相关(性别交互作用 P 值<0.0001)。胆固醇吸收标志物在女性或男性中均不能预测 HCHD 或全因 CVD。
这些数据表明,胆固醇合成标志物和 HCHD(特别是冠心病死亡和心肌梗死发生率)的 10 年预后价值在性别上存在显著差异。