Division of Nephrology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
PLoS One. 2013;8(3):e60008. doi: 10.1371/journal.pone.0060008. Epub 2013 Mar 20.
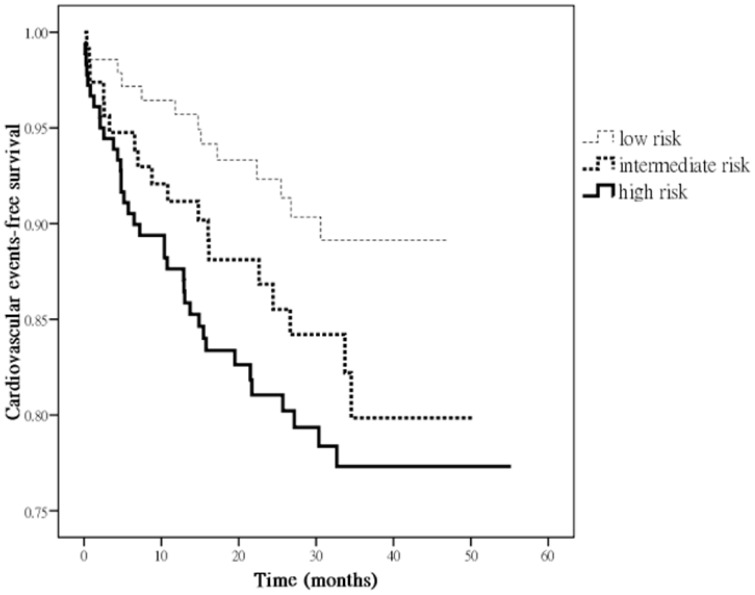
The Framingham Risk Score (FRS) was developed to predict coronary heart disease in various populations, and it tended to under-estimate the risk in chronic kidney disease (CKD) patients. Our objectives were to determine whether FRS was associated with cardiovascular events, and to evaluate the role of new risk markers and echocardiographic parameters when they were added to a FRS model. This study enrolled 439 CKD patients. The FRS is used to identify individuals categorically as "low" (<10% of 10-year risk), "intermediate" (10-20% risk) or "high" risk (≥ 20% risk). A significant improvement in model prediction was based on the -2 log likelihood ratio statistic and c-statistic. "High" risk (v.s. "low" risk) predicts cardiovascular events either without (hazard ratios [HR] 2.090, 95% confidence interval [CI] 1.144 to 3.818) or with adjustment for clinical, biochemical and echocardiographic parameters (HR 1.924, 95% CI 1.008 to 3.673). Besides, the addition of albumin, hemoglobin, estimated glomerular filtration rate, proteinuria, left atrial diameter >4.7 cm, left ventricular hypertrophy or left ventricular ejection fraction<50% to the FRS model significantly improves the predictive values for cardiovascular events. In CKD patients, "high" risk categorized by FRS predicts cardiovascular events. Novel biomarkers and echocardiographic parameters provide additional predictive values for cardiovascular events. Future study is needed to assess whether risk assessment enhanced by using these biomarkers and echocardiographic parameters might contribute to more effective prediction and better care for patients.
弗雷明汉风险评分(Framingham Risk Score,FRS)用于预测不同人群的冠心病,并且在慢性肾脏病(Chronic Kidney Disease,CKD)患者中往往低估了风险。我们的目的是确定 FRS 是否与心血管事件相关,并评估新的风险标志物和超声心动图参数在加入 FRS 模型时的作用。这项研究纳入了 439 名 CKD 患者。FRS 用于将个体分为“低危”(<10%的 10 年风险)、“中危”(10-20%风险)或“高危”(≥20%风险)。基于-2 对数似然比统计量和 c 统计量,模型预测得到显著改善。“高危”(与“低危”相比)预测心血管事件,无论是在不调整(危险比[HR]2.090,95%置信区间[CI]1.144 至 3.818)还是调整临床、生化和超声心动图参数的情况下(HR 1.924,95%CI1.008 至 3.673)。此外,将白蛋白、血红蛋白、估计肾小球滤过率、蛋白尿、左心房直径>4.7cm、左心室肥厚或左心室射血分数<50%等参数加入 FRS 模型,可显著提高心血管事件的预测值。在 CKD 患者中,FRS 分类的“高危”预测心血管事件。新型生物标志物和超声心动图参数为心血管事件提供了额外的预测价值。需要进一步研究评估是否使用这些生物标志物和超声心动图参数进行风险评估可提高预测效果和改善患者治疗。