Department of Neurology, Maastricht University Medical Centre, Maastricht, The Netherlands.
BMJ Open. 2013 Apr 2;3(4). doi: 10.1136/bmjopen-2013-002613. Print 2013.
Numerous ultrasound studies have suggested that a typical enlarged area of echogenicity in the substantia nigra (SN+) can help diagnose idiopathic Parkinson's disease (IPD). Almost all these studies were retrospective and involved patients with well-established diagnoses and long-disease duration. In this study the diagnostic accuracy of transcranial sonography (TCS) of the substantia nigra in the patient with an undiagnosed parkinsonian syndrome of recent onset has been evaluated.
Prospective cohort study for diagnostic accuracy.
Neurology outpatient clinics of two teaching hospitals in the Netherlands.
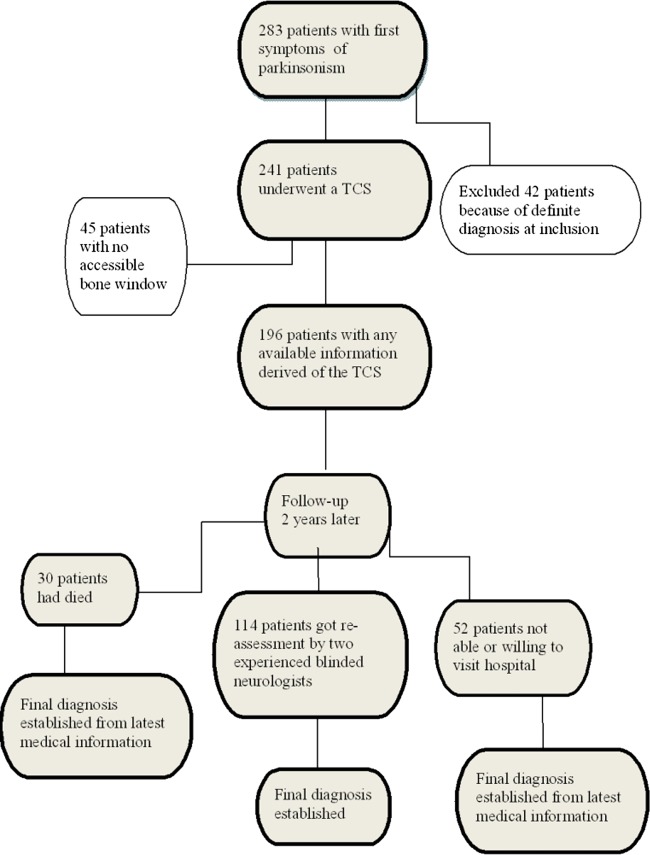
196 consecutive patients, who were referred to two neurology outpatient clinics for analysis of clinically unclear parkinsonism. Within 2 weeks of inclusion all patients also underwent a TCS and a (123)I-ioflupane Single Photon Emission CT (FP-CIT SPECT) scan of the brain (n=176).
After 2 years, patients were re-examined by two movement disorder specialist neurologists for a final clinical diagnosis, that served as a surrogate gold standard for our study.
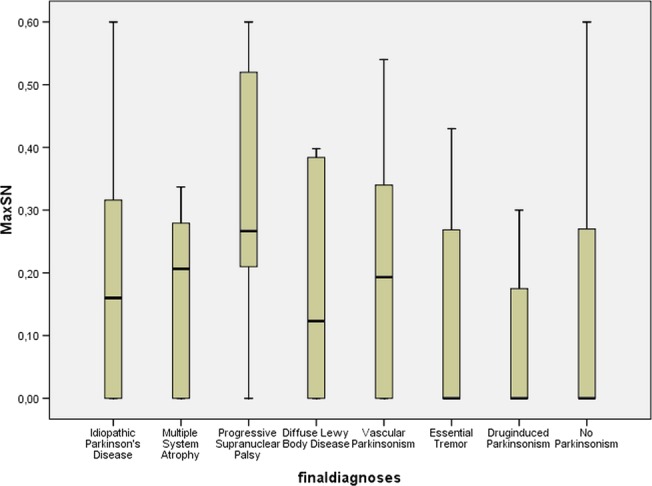
Temporal acoustic windows were insufficient in 45 of 241 patients (18.67%). The final clinical diagnosis was IPD in 102 (52.0%) patients. Twenty-four (12.3%) patients were diagnosed with atypical parkinsonisms (APS) of which 8 (4.0%) multisystem atrophy (MSA), 6 (3.1%) progressive supranuclear palsy (PSP), 6 (3.1%) Lewy body dementia and 4 (2%) corticobasal degeneration. Twenty-one (10.7%) patients had a diagnosis of vascular parkinsonism, 20 (10.2%) essential tremor, 7 (3.6%) drug-induced parkinsonism and 22 (11.2%) patients had no parkinsonism but an alternative diagnosis. The sensitivity of a SN+ for the diagnosis IPD was 0.40 (CI 0.30 to 0.50) and the specificity 0.61 (CI 0.52 to 0.70). Hereby the positive predictive value (PPV) was 0.53 and the negative predictive value (NPV) 0.48. The sensitivity and specificity of FP-CIT SPECT scans for diagnosing IPD was 0.88 (CI 0.1 to 0.95) and 0.68 (CI 0.58 to 0.76) with a PPV of 0.75 and an NPV of 0.84.
The diagnostic accuracy of TCS in early stage Parkinson's disease is not sufficient for routine clinical use. CLINICALTRIALS.GOV IDENTIFIER: NCT0036819.
许多超声研究表明,黑质(SN+)中典型的回声增强区域有助于诊断特发性帕金森病(IPD)。几乎所有这些研究都是回顾性的,涉及到已确诊且疾病病程较长的患者。在这项研究中,评估了经颅超声(TCS)对新近发病的帕金森综合征患者的诊断准确性。
前瞻性队列研究,用于诊断准确性评估。
荷兰两家教学医院的神经内科门诊。
196 名连续患者,因临床不明确的帕金森病被转诊至两家神经内科门诊进行分析。在纳入后的 2 周内,所有患者还接受了 TCS 和(123)I-ioflupane 单光子发射计算机断层扫描(FP-CIT SPECT)脑扫描(n=176)。
2 年后,由两名运动障碍专家神经病学家对患者进行重新检查,以获得最终临床诊断,该诊断作为本研究的替代金标准。
241 名患者中有 45 名(18.67%)的颞窗不足。最终临床诊断为 102 名(52.0%)患者为 IPD。24 名(12.3%)患者被诊断为非典型帕金森病(APS),其中 8 名(4.0%)为多系统萎缩(MSA),6 名(3.1%)为进行性核上性麻痹(PSP),6 名(3.1%)为路易体痴呆,4 名(2%)为皮质基底节变性。21 名(10.7%)患者为血管性帕金森病,20 名(10.2%)为特发性震颤,7 名(3.6%)为药物诱导的帕金森病,22 名(11.2%)患者无帕金森病,但有其他诊断。SN+对 IPD 的诊断敏感性为 0.40(95%CI 0.30 至 0.50),特异性为 0.61(95%CI 0.52 至 0.70)。因此,阳性预测值(PPV)为 0.53,阴性预测值(NPV)为 0.48。FP-CIT SPECT 扫描对 IPD 的诊断的敏感性和特异性分别为 0.88(95%CI 0.1 至 0.95)和 0.68(95%CI 0.58 至 0.76),PPV 为 0.75,NPV 为 0.84。
TCS 在早期帕金森病中的诊断准确性不足以用于常规临床应用。临床试验.gov 标识符:NCT0036819。