Master of International Health Management, Economics and Policy Program, SDA Bocconi School of Management, Milan, Italy.
PLoS One. 2013;8(3):e57778. doi: 10.1371/journal.pone.0057778. Epub 2013 Mar 12.
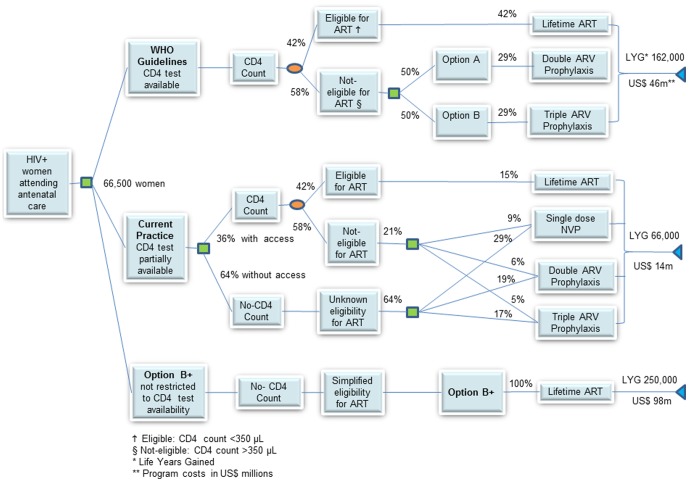
The Ministry of Health in Malawi is implementing a pragmatic and innovative approach for the management of all HIV-infected pregnant women, termed Option B+, which consists of providing life-long antiretroviral treatment, regardless of their CD4 count or clinical stage. Our objective was to determine if Option B+ represents a cost-effective option.
A decision model simulates the disease progression of a cohort of HIV-infected pregnant women receiving prophylaxis and antiretroviral therapy, and estimates the number of paediatric infections averted and maternal life years gained over a ten-year time horizon. We assess the cost-effectiveness from the Ministry of Health perspective while taking into account the practical realities of implementing ART services in Malawi.
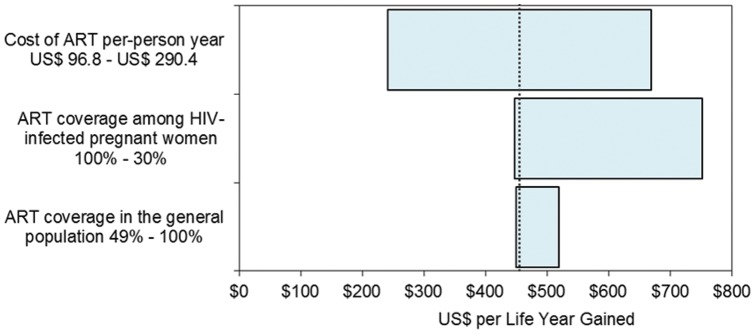
If implemented as recommended by the World Health Organization, options A, B and B+ are equivalent in preventing new infant infections, yielding cost effectiveness ratios between US$ 37 and US$ 69 per disability adjusted life year averted in children. However, when the three options are compared to the current practice, the provision of antiretroviral therapy to all mothers (Option B+) not only prevents infant infections, but also improves the ten-year survival in mothers more than four-fold. This translates into saving more than 250,000 maternal life years, as compared to mothers receiving only Option A or B, with savings of 153,000 and 172,000 life years respectively. Option B+ also yields favourable incremental cost effectiveness ratios (ICER) of US$ 455 per life year gained over the current practice.
In Malawi, Option B+ represents a favorable policy option from a cost-effectiveness perspective to prevent future infant infections, save mothers' lives and reduce orphanhood. Although Option B+ would require more financial resources initially, it would save societal resources in the long-term and represents a strategic option to simplify and integrate HIV services into maternal, newborn and child health programmes.
马拉维卫生部正在实施一种务实且创新的方法来管理所有感染 HIV 的孕妇,称为 B 方案+,其中包括提供终身抗逆转录病毒治疗,而不论其 CD4 计数或临床阶段如何。我们的目的是确定 B 方案+是否代表一种具有成本效益的选择。
决策模型模拟了接受预防和抗逆转录病毒治疗的 HIV 感染孕妇队列的疾病进展,并估计了在十年时间内避免多少儿童感染以及获得多少产妇生命年。我们从卫生部的角度评估成本效益,同时考虑到在马拉维实施抗逆转录病毒治疗服务的实际情况。
如果按照世界卫生组织的建议实施,A、B 和 B+方案在预防新的婴儿感染方面效果相同,在儿童每获得一个残疾调整生命年的成本效益比为 37 至 69 美元之间。然而,当将这三种方案与当前实践进行比较时,为所有母亲提供抗逆转录病毒治疗(B 方案+)不仅可以预防婴儿感染,而且还使母亲在十年内的存活率提高四倍以上。与仅接受 A 或 B 方案的母亲相比,这意味着可以节省超过 25 万个母亲的生命年,分别节省 15.3 万和 17.2 万生命年。B 方案+相对于当前实践,还具有 455 美元的增量成本效益比(ICER)优势,每获得一个生命年的收益。
在马拉维,从成本效益的角度来看,B 方案+代表了一种有利的政策选择,可以预防未来的婴儿感染,拯救母亲的生命并减少孤儿人数。虽然 B 方案+最初需要更多的财政资源,但从长期来看,它将节省社会资源,是将 HIV 服务简化并整合到母婴和儿童健康方案中的一种战略选择。