Medical Practice Evaluation Center, Divisions of Infectious Disease, Massachusetts General Hospital, Boston, MA 02114, USA.
Clin Infect Dis. 2013 Feb;56(3):430-46. doi: 10.1093/cid/cis858. Epub 2012 Nov 30.
In 2010, the World Health Organization (WHO) released revised guidelines for prevention of mother-to-child human immunodeficiency virus (HIV) transmission (PMTCT). We projected clinical impacts, costs, and cost-effectiveness of WHO-recommended PMTCT strategies in Zimbabwe.
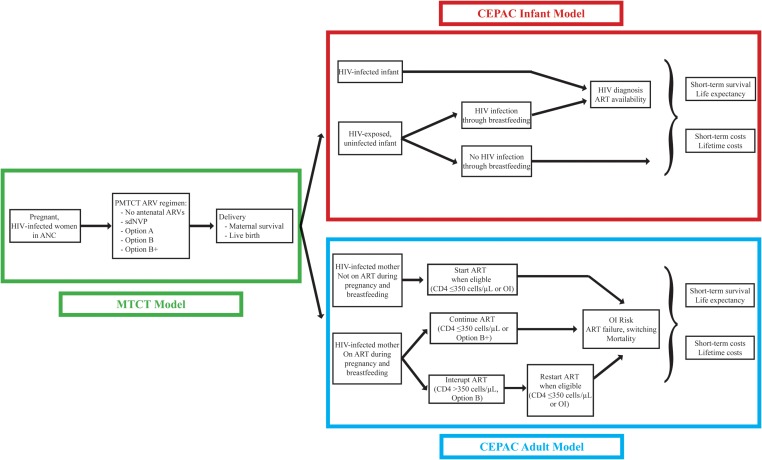
We used Zimbabwean data in a validated computer model to simulate a cohort of pregnant, HIV-infected women (mean age, 24 years; mean CD4 count, 451 cells/µL; subsequent 18 months of breastfeeding). We simulated guideline-concordant care for 4 PMTCT regimens: single-dose nevirapine (sdNVP); WHO-recommended Option A, WHO-recommended Option B, and Option B+ (lifelong maternal 3-drug antiretroviral therapy regardless of CD4). Outcomes included maternal and infant life expectancy (LE) and lifetime healthcare costs (2008 US dollars [USD]). Incremental cost-effectiveness ratios (ICERs, in USD per year of life saved [YLS]) were calculated from combined (maternal + infant) discounted costs and LE.
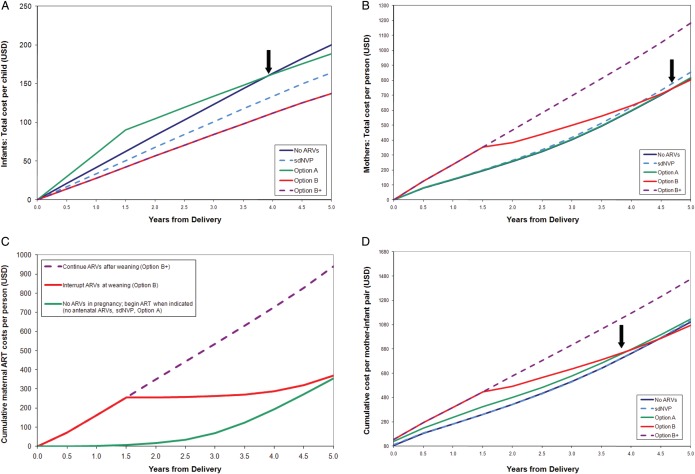
Replacing sdNVP with Option A increased combined maternal and infant LE from 36.97 to 37.89 years and would reduce lifetime costs from $5760 to $5710 per mother-infant pair. Compared with Option A, Option B further improved LE (38.32 years), and saved money within 4 years after delivery ($5630 per mother-infant pair). Option B+ (LE, 39.04 years; lifetime cost, $6620 per mother-infant pair) improved maternal and infant health, with an ICER of $1370 per YLS compared with Option B.
Replacing sdNVP with Option A or Option B will improve maternal and infant outcomes and save money; Option B increases health benefits and decreases costs compared with Option A. Option B+ further improves maternal outcomes, with an ICER (compared with Option B) similar to many current HIV-related healthcare interventions.
2010 年,世界卫生组织(WHO)发布了修订后的预防母婴传播人免疫缺陷病毒(HIV)指南(PMTCT)。我们预测了 WHO 推荐的 PMTCT 策略在津巴布韦的临床影响、成本和成本效益。
我们使用津巴布韦的数据在经过验证的计算机模型中模拟了一组感染 HIV 的孕妇(平均年龄 24 岁;平均 CD4 计数 451 个/µL;随后 18 个月母乳喂养)。我们模拟了 4 种 PMTCT 方案的指南一致护理:单剂量奈韦拉平(sdNVP);WHO 推荐的 A 方案、WHO 推荐的 B 方案和 B+方案(无论 CD4 如何,终生接受 3 种抗逆转录病毒药物治疗)。结果包括母婴预期寿命(LE)和终生医疗保健成本(2008 年美元[USD])。从合并(母婴)贴现成本和 LE 中计算出增量成本效益比(ICER,每年每节省 1 个生命的成本[YLS])。
用 A 方案取代 sdNVP 将母婴联合预期寿命从 36.97 年增加到 37.89 年,并将每个母婴对的终生成本从 5760 美元降低到 5710 美元。与 A 方案相比,B 方案进一步提高了 LE(38.32 年),并在分娩后 4 年内节省了资金(每个母婴对 5630 美元)。B+方案(LE,39.04 年;终生成本,每个母婴对 6620 美元)改善了母婴健康,与 B 方案相比,ICER 为 1370 美元/YLS。
用 A 方案或 B 方案取代 sdNVP 将改善母婴结局并节省资金;与 A 方案相比,B 方案增加了健康益处并降低了成本。B+方案进一步提高了母亲的结局,与 B 方案相比,其 ICER(与 B 方案相比)与许多当前的 HIV 相关医疗保健干预措施相似。