Kaseda Yumiko, Yamawaki Takemori, Ikeda Junko, Hayata Miwa, Dohi Eisuke, Ohshita Tomohiko, Ochi Kazuhide, Nomura Eiichi, Matsumoto Masayasu
Department of Neurology, Hiroshima City General Rehabilitation Center, Hiroshima University Graduate School of Biomedical Sciences, Hiroshima, Japan.
Case Rep Neurol. 2013 Mar 29;5(1):68-73. doi: 10.1159/000350434. Print 2013 Jan.
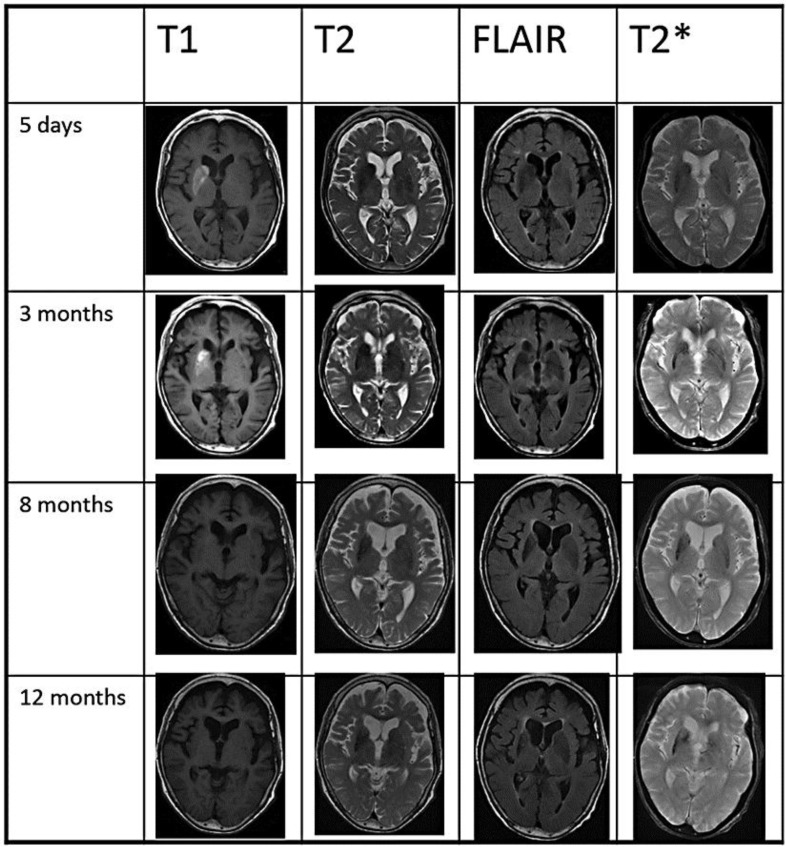
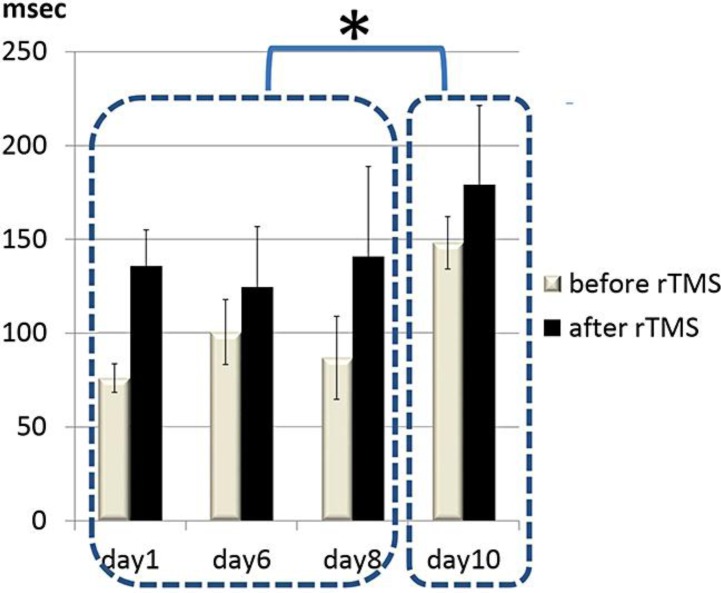
Diabetic hemichorea-hemiballism with non-ketotic hyperglycemia is usually a benign syndrome. Here, we report a 78-year-old woman with persistent hemichorea (HC) for longer than 1 year with a recurrence after rapid correction of hyperglycemia. Following the disappearance of the characteristic T1 hyperintensity at 3 months after onset, an MRI demonstrated T2* hypointensity and atrophic changes in the contralateral striatum, suggesting irreversible neuronal loss and some vascular proliferation. The electrophysiological examination using transcranial magnetic stimulation revealed significantly shorter cortical silent periods (CSPs) on the contralateral primary motor cortex (M1), possibly in relation to cortical hyperexcitability. We have applied 10 daily sessions of low-frequency repetitive transcranial magnetic stimulation (rTMS) over the contralateral M1 to reduce the hyperexcitability. The HC was suppressed during and for several minutes after rTMS with prolongation of CSPs. After rehabilitation therapy, the patient was able to walk independently with a walker. We suggest that the combination of low-frequency rTMS and rehabilitation therapy may be a possible choice in medically refractory involuntary movements.
非酮症高血糖性糖尿病性偏侧舞蹈症-偏侧投掷症通常是一种良性综合征。在此,我们报告一名78岁女性,持续性偏侧舞蹈症(HC)超过1年,在血糖快速纠正后复发。发病3个月后特征性T1高信号消失,MRI显示对侧纹状体T2*低信号和萎缩性改变,提示不可逆的神经元丢失和一些血管增生。经颅磁刺激的电生理检查显示,对侧初级运动皮层(M1)的皮质静息期(CSP)明显缩短,可能与皮质兴奋性过高有关。我们在对侧M1上进行了10次每日低频重复经颅磁刺激(rTMS),以降低兴奋性过高。rTMS期间及之后几分钟HC得到抑制,CSP延长。经过康复治疗,患者能够借助助行器独立行走。我们认为低频rTMS与康复治疗相结合可能是药物难治性不自主运动的一种可能选择。