Zhao Xiaojing, Qian Liqiang, Luo Qingquan, Huang Jia
Shanghai Lung Cancer Center/Shanghai Chest Hospital, 241 West HuaiHai Road, Shanghai, China.
J Cardiothorac Surg. 2013 Apr 29;8:116. doi: 10.1186/1749-8090-8-116.
While video-assisted thoracic surgery lobectomy has been widely accepted for the treatment of non-small cell lung cancer, the debate over video-assisted thoracic surgery segmentectomy still remains. This study compared the clinical outcomes using the two procedures for stage I non-small cell lung cancer patients.
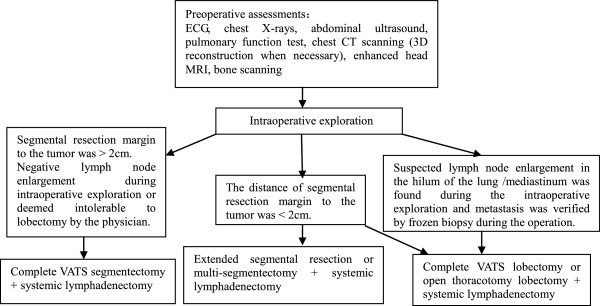
Retrospective review was conducted on patients who underwent video-assisted thoracic surgery segmentectomy or lobectomy for clinical stage I non-small cell lung cancer at Shanghai Chest Hospital between November 2009 and May 2012. Video-assisted thoracic surgery segmentectomy was performed on 36 patients and video-assisted thoracic surgery lobectomy on 138 patients. Comparisons between the 2 groups were performed in patient demographic and clinical characteristics, intraoperative parameters and oncology outcomes.
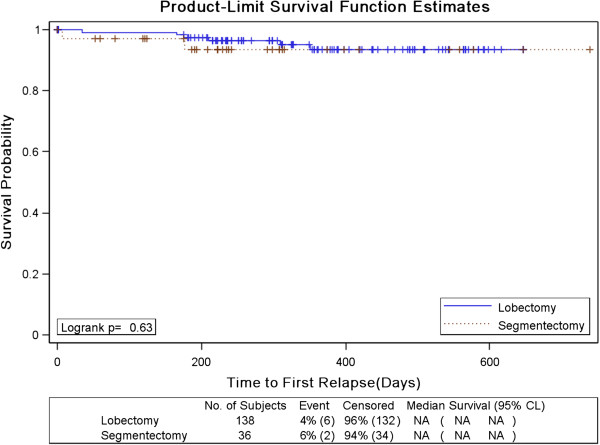
Mean volume of chest tube drainage after operation was smaller for segmentectomy than for lobectomy (1021 ml vs. 1328 ml, P=0.036). Other parameters analysis including blood loss, operation time, chest tube duration and length of hospital stay favors the segmentectomy group numerically without significance. There was no significant difference in distributions in both intra and post operative complications. There was one peri-operative mortality from segmentectomy group and all other patients are alive with a median follow up of 327 days. There were 1 (2.8%) locoregional recurrence after segmentectomy and 6 recurrences (4.4%) after lobectomy (P=1.00). Multivariate survival analysis revealed no significant difference in recurrence-free survivals between the two groups. Two patients successfully underwent bilateral segmentectomies and are free of disease.
For patients with stage I non-small cell lung cancer, video-assisted thoracic surgery segmentectomy offers a safe and equally effective option and can be applied to complicated operation such as bilateral segmentectomy.
虽然电视辅助胸腔镜肺叶切除术已被广泛接受用于治疗非小细胞肺癌,但关于电视辅助胸腔镜肺段切除术的争论仍然存在。本研究比较了这两种手术方法用于I期非小细胞肺癌患者的临床疗效。
对2009年11月至2012年5月在上海胸科医院接受电视辅助胸腔镜肺段切除术或肺叶切除术治疗临床I期非小细胞肺癌的患者进行回顾性研究。36例患者接受电视辅助胸腔镜肺段切除术,138例患者接受电视辅助胸腔镜肺叶切除术。对两组患者的人口统计学和临床特征、术中参数及肿瘤学结局进行比较。
肺段切除术术后胸腔引流管平均引流量低于肺叶切除术(1021 ml对1328 ml,P = 0.036)。包括失血量、手术时间、胸腔引流管留置时间和住院时间在内的其他参数分析在数值上有利于肺段切除术组,但无统计学意义。术中和术后并发症的分布无显著差异。肺段切除术组有1例围手术期死亡,所有其他患者均存活,中位随访时间为327天。肺段切除术后有1例(2.8%)局部区域复发,肺叶切除术后有6例(4.4%)复发(P = 1.00)。多因素生存分析显示两组间无复发生存率的显著差异。2例患者成功接受双侧肺段切除术,且无疾病复发。
对于I期非小细胞肺癌患者,电视辅助胸腔镜肺段切除术是一种安全且同样有效的选择,可应用于如双侧肺段切除术等复杂手术。