Department of Pathology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; Department of Health Policy and Management, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; Department of Pathology, Brigham and Women's Hospital, Boston, Massachusetts.
Transfusion. 2014 Jan;54(1):86-97. doi: 10.1111/trf.12250. Epub 2013 May 21.
Sickle cell disease is associated with extensive health care utilization; estimated lifetime costs exceed $460,000 per patient. Approximately 30% of chronically transfused sickle cell patients become alloimmunized to red blood cell antigens, but these patients cannot be identified a priori. Prospective antigen matching can prevent alloimmunization, but is costly and may not benefit most patients.
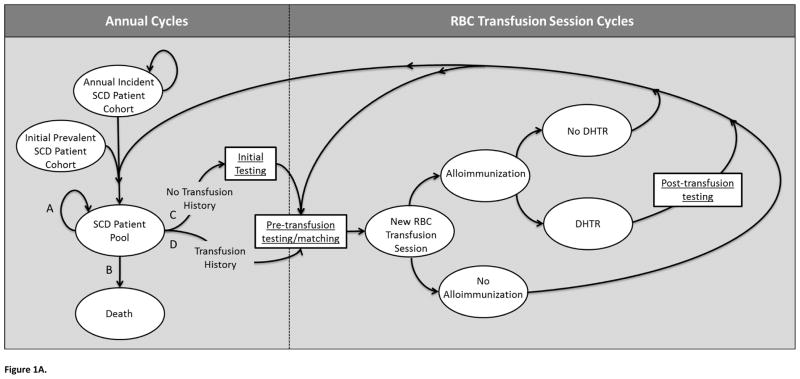
A Markov-based model was constructed to compare the health and financial implications of four alternative antigen-matching strategies for chronically transfused sickle cell patients. The strategies varied by the group of patients receiving matched blood (all patients prophylactically or only patients with a history of alloimmunization [history-based]), and by the extent of antigen matching (limited to C, E, and K, or extended to 11 antigens). Direct medical costs and alloimmunization events were assessed over 10- and 20-year periods, for a hypothetical cohort of initially transfusion-naive patients and for a dynamic population.
Within a hypothetical cohort of initially transfusion-naive patients, implementing prophylactic limited matching for all chronically transfused patients instead of history-based limited matching is expected to cost an additional $765.56 million over 10 years, but result in 2072 fewer alloimmunization events. Within the same cohort, implementing prospective extensive matching is expected to cost $1.86 billion more than history-based extensive matching, but result in 2424 fewer alloimmunization events. Averting a single alloimmunization event using prospective matching would cost $369,482 to $769,284. Among a dynamic population over 10 years, prospective limited matching is expected to cost $358.34 million more than history-based limited matching.
While prospective matching for all transfused patients would reduce alloimmunization, this strategy requires considerable expenditure.
镰状细胞病与广泛的医疗保健利用有关;估计每位患者的终身费用超过 46 万美元。大约 30%的慢性输血镰状细胞病患者对红细胞抗原产生同种免疫,但这些患者不能事先确定。前瞻性抗原匹配可以预防同种免疫,但成本高昂,可能对大多数患者无益。
构建了一个基于马尔可夫模型的模型,以比较四种替代慢性输血镰状细胞病患者抗原匹配策略的健康和财务影响。这些策略因接受匹配血液的患者群体而异(所有患者预防性接受或仅接受同种免疫史的患者接受),以及抗原匹配的程度而异(仅限于 C、E 和 K,或扩展到 11 个抗原)。在 10 年和 20 年期间,评估了假设的初始无输血患者队列和动态人群的直接医疗费用和同种免疫事件。
在初始无输血的假设队列中,与基于历史的有限匹配相比,对所有慢性输血患者实施预防性有限匹配预计在 10 年内将额外增加 7.6556 亿美元的成本,但将减少 2072 次同种免疫事件。在同一队列中,与基于历史的广泛匹配相比,实施前瞻性广泛匹配预计将增加 18.6 亿美元的成本,但将减少 2424 次同种免疫事件。使用前瞻性匹配来避免单次同种免疫事件的成本为 369,482 美元至 769,284 美元。在 10 年内的动态人群中,与基于历史的有限匹配相比,前瞻性有限匹配预计将增加 3.5834 亿美元的成本。
虽然对所有输血患者进行前瞻性匹配可以减少同种免疫,但这种策略需要大量支出。