Ramirez-Avila Lynn, Noubary Farzad, Pansegrouw Deirdre, Sithole Siphesihle, Giddy Janet, Losina Elena, Walensky Rochelle P, Bassett Ingrid V
From the *Division of Infectious Diseases, Children's Hospital Boston, Boston, MA; †Division of Pediatric Infectious Disease, UCLA School of Medicine, Los Angeles, CA; ‡Medical Practice Evaluation Center; §Division of General Medicine, Massachusetts General Hospital, Boston, MA; ¶McCord Hospital, Durban, KwaZulu Natal, South Africa; ‖Department of Orthopedic Surgery; **Division of Rheumatology, Brigham and Women's Hospital; ††Department of Biostatistics, Boston University, Boston; ‡‡Center for AIDS Research, Harvard Medical School, Cambridge; §§Division of Infectious Disease, Brigham and Women's Hospital; and ¶¶Division of Infectious Diseases, Massachusetts General Hospital, Boston, MA.
Pediatr Infect Dis J. 2013 Dec;32(12):1348-53. doi: 10.1097/INF.0b013e31829ba34b.
Limited access to HIV testing of children impedes early diagnosis and access to antiretroviral therapy. Our objective was to evaluate the feasibility and acceptability of routine pediatric HIV testing in an urban, fee-for-service, outpatient clinic in Durban, South Africa.
We assessed the number of patients (0-15 years) who underwent HIV testing upon physician referral during a baseline period. We then established a routine, voluntary HIV testing study for pediatric patients, regardless of symptoms. Parents/caretakers were offered free rapid fingerstick HIV testing of their child. For patients <18 months, the biological mother was offered HIV testing and HIV DNA polymerase chain reaction was used to confirm the infant's status. The primary outcome was the HIV testing yield, defined as the average number of positive tests per month during the routine compared with the baseline period.
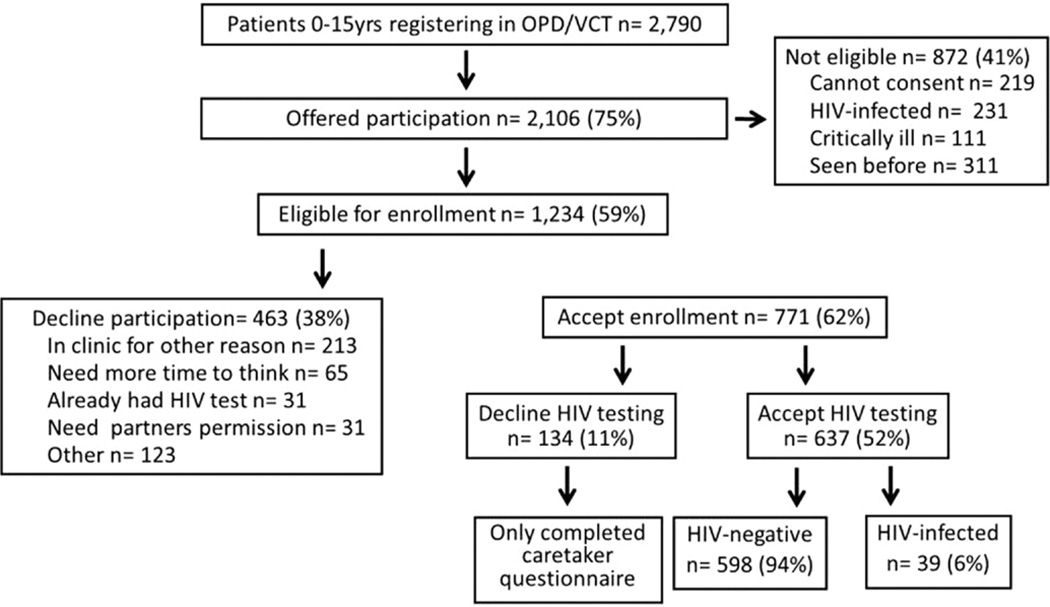
Over a 5-month baseline testing period, 931 pediatric patients registered for outpatient care. Of the 124 (13%) patients who underwent testing on physician referral, 21 (17%, 95% confidence interval: 11-25%) were HIV infected. During a 13-month routine testing period, 2790 patients registered for care and 2106 (75%) were approached for participation. Of these, 1234 were eligible and 771 (62%) enrolled. Among those eligible, 637 (52%, 95% confidence interval: 49-54%) accepted testing of their child or themselves (biological mothers of infants <18 months). There was an increase in the average number of HIV tests during the routine compared with the baseline HIV testing periods (49 versus 25 tests/month, P = 0.001) but no difference in the HIV testing yield during the testing periods (3 versus 4 positive HIV tests/month, P = 0.06). However, during the routine testing period, HIV prevalence remains extraordinarily high with 39 (6%, 95% confidence interval: 4-8%) newly diagnosed HIV-infected children (median 7 years, 56% female).
Targeted and symptom-based testing referral identifies an equivalent number of HIV-infected children as routine HIV testing. Routine HIV testing identifies a high burden of HIV and is a feasible and moderately acceptable strategy in an outpatient clinic in a high prevalence area.
儿童获得HIV检测的机会有限,这阻碍了早期诊断及抗逆转录病毒治疗的获取。我们的目标是评估在南非德班一家按服务收费的城市门诊诊所开展常规儿科HIV检测的可行性和可接受性。
我们评估了在基线期因医生转诊而接受HIV检测的患者(0至15岁)数量。然后,我们为儿科患者建立了一项常规的自愿HIV检测研究,无论其有无症状。为家长/监护人提供为其孩子免费进行快速指尖HIV检测。对于18个月以下的患者,为其生母提供HIV检测,并使用HIV DNA聚合酶链反应来确认婴儿的状况。主要结局是HIV检测阳性率,定义为常规检测期间与基线期相比每月阳性检测的平均数量。
在为期5个月的基线检测期内,931名儿科患者登记接受门诊护理。在因医生转诊而接受检测的124名(13%)患者中,21名(17%,95%置信区间:11% - 25%)感染了HIV。在为期13个月的常规检测期内,2790名患者登记接受护理,其中2106名(75%)被邀请参与。其中,1234名符合条件,771名(62%)登记参加。在符合条件的人群中,637名(52%,95%置信区间:49% - 54%)接受了为其孩子或自身(18个月以下婴儿的生母)的检测。与基线HIV检测期相比,常规检测期HIV检测的平均数量有所增加(每月49次检测对25次检测,P = 0.001),但检测期内HIV检测阳性率无差异(每月3次对4次HIV阳性检测,P = 0.06)。然而,在常规检测期内,HIV患病率仍然极高,有39名(6%,95%置信区间:4% - 8%)新诊断的HIV感染儿童(中位年龄7岁,56%为女性)。
针对性的基于症状的检测转诊所发现的HIV感染儿童数量与常规HIV检测相当。常规HIV检测发现HIV负担较重,并且在高流行地区的门诊诊所是一种可行且有一定可接受性的策略。